This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
With this longer lifespan, calcific aortic stenosis (AS) was identified as an emerging critical risk factor for cardiac death in older patients. Intervention to relieve critical AS has the potential for immediate improvement in healthspan and lifespan. years by 4.3 years (30%).
These two acquisitions could impact Edwards’ structural heart and heart failure portfolios in unique and meaningful ways… JenaValve’s Trilogy TAVR system doesn’t yet have FDA approval, but is CE Marked for both aortic regurgitation and aortic stenosis, which is notable given that all other TAVR systems only address aortic stenosis.
The software generates accurate reports in minutes using inexpensive devices, enabling emergency medicine, criticalcare, internal medicine, hospitalists and primary care physicians to make informed care decisions at the bedside.
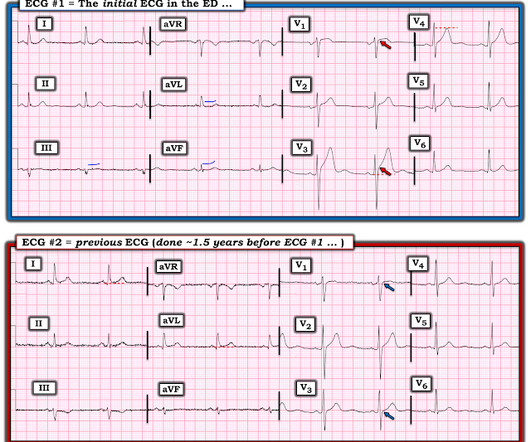
It turns out that the conventional algorithm was also worried, and because of that, the patient was brought to the criticalcare area. The STE in V1 is out of proportion to the S-wave, so V1 is also very worrisome (something I did not see on my phone). So we don't have a good idea how large the final infarct size was.
The patient was moved to the criticalcare area (stabilization room). Angiogram Culprit Lesion (s): ST elevation myocardial infarction due to 99% stenosis of the distal LAD Formal echo: Normal estimated left ventricular ejection fraction, 63%. Cath lab was activated. A 2nd ECG recorded 50 minutes after the first.
Angiogram --LAD is a large-caliber vessel that wraps around the apex --There is a tubular 80% in the ostial LAD that was relatively smooth but did not resolve with repeated doses of IC nitroglycerin --There is a tiny D1, medium D2, and small D3 Lesion on Prox LAD: Ostial 80% stenosis. Pre- procedure TIMI III flow was noted.
Another very astute faculty physician immediately recognized that the ECG is diagnostic of posterior and lateral OMI , and activated the cath lab. The cardiology fellow came to the ED. Supplies a very large OM1.
There was high suspicion of OMI, so patient was brought to criticalcare area and another ECG was recorded just 7 minutes later as the pain had diminished to 4/10. Left main: no significant stenosis. LAD: proximal 60% eccentric stenosis the hemodynamic significance of which is indeterminate.
Colin is an emergency medicine resident beginning his criticalcare fellowship in the summer with a strong interest in the role of ECG in criticalcare and OMI. Written by Colin Jenkins. Edits by Willy Frick. This suggests thrombus (since the contrast does not penetrate the formed thrombus very well).
A 3rd troponin returned before the angiogram was done and was 2956 ng/L Here is the angiogram description: The distal RCA has mild diffuse disease and bifurcates to give a large RPDA which is without significant stenosis. Plus he did a 2 year combined EM Cardiology and CriticalCare Fellowship.
This EKG was recorded as part of a standing order for criticalcare. He had been smoking an opiate and suddenly collapsed. He was ventilated with BVM on arrival. He awoke with naloxone. He denied any CP or SOB. An EKG was repeated at 5 minutes The T-wave is less hyperacute. Maybe there is some spontaneous reperfusion?
Later, I was working in the ED and a patient was moved from a regular room to the criticalcare area due to recurrent hypotension. The patient was now under my care. That condition is tricuspid stenosis, which is rare. So I thought it probably is not posterior OMI and I just moved on and kept reading EKGs.
The patient arrived at the Emergency Dept criticalcare area and had this ECG recorded: The sinus bradycardia persists. He was taken to the cath lab and underwent emergent intervention: Thrombotic stenosis of the proximal RCA (95% with evidence of plaque rupture) is the culprit for the patient's inferoposterior STEMI.
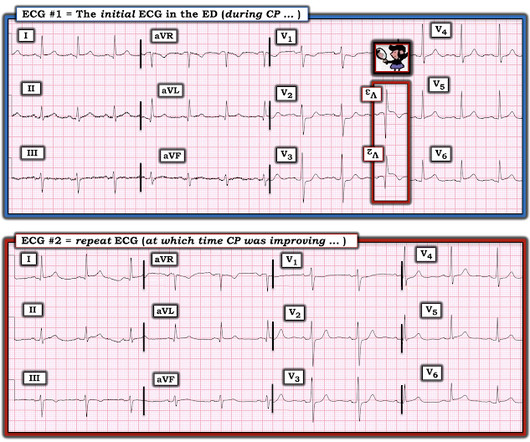
We brought the patient into one of our criticalcare rooms and immediately got more history while recording this repeat ECG: The STE in I has greatly diminished or entirely disappeared. Let's zoom in on I and aVL: Lead I (top panel) has less than 1mm of STE. aVL is also less dramatic but still abnormal.
Adult Cardiac Surgery Database Lead Author Title Publication Date Jacob Raphael Red Blood Cell Transfusion and Pulmonary Complications: The Society of Thoracic Surgeons Adult Cardiac Surgery Database Analysis The Annals of Thoracic Surgery January 2024 Joseph Sabik Multi-Arterial versus Single-Arterial Coronary Surgery: Ten Year Follow-up of One Million (..)
Mark Erfe 2 Outcomes of Sutureless/Rapid Deployment Valves Compared to Traditional Bioprosthetic Aortic Valves The Annals of Thoracic Surgery September 2020 Victor Nauffal 2 Short-Term Outcomes of Transcatheter Versus Isolated Surgical Aortic Valve Replacement for Mediastinal Radiation-Associated Severe Aortic Stenosis Circulation: Cardiovascular Interventions (..)
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


















Let's personalize your content