This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
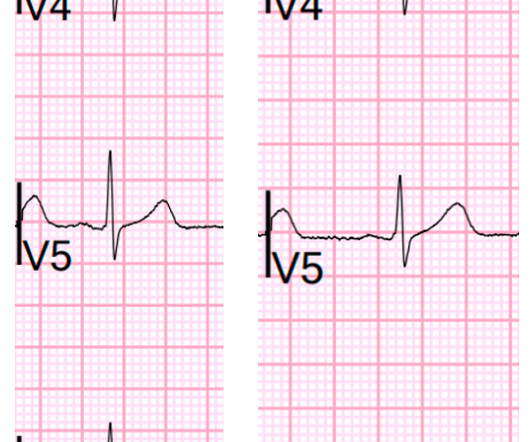
I immediately activated the criticalcare team and walked the patient to the criticalcare area, our "Stabilization Room." Acute MI due to plaque rupture does happen in young people, including young women. There are relatively large T-waves in V4-V6. Let's record another one." Beware a low HEART score.
Given the presentation, the cardiologist stented the vessel and the patient returned to the ICU for ongoing criticalcare. Lesions less than 70% are generally considered to be non-flow limiting. Two subsequent troponins were down trending. Echocardiogram showed LVEF 66% with normal wall motion and normal diastolic function.
Session 508) Battle of the Imagers - Jeopardy Edition! Session 509) Who Wants to Be a Millionaire in Eradicating Vascular Medicine Disparities? Clinical and Investigative Horizons The Clinical and Investigative Horizons is a new type of late-breaker session that was added for ACC23 and is back by popular demand.
Colin is an emergency medicine resident beginning his criticalcare fellowship in the summer with a strong interest in the role of ECG in criticalcare and OMI. As an aside, the LCx OMI is a type 2 event, since it is due to supply-demand mismatch from thrombus, and not due to atherosclerotic plaque rupture or erosion).
The patient arrived at the Emergency Dept criticalcare area and had this ECG recorded: The sinus bradycardia persists. He was taken to the cath lab and underwent emergent intervention: Thrombotic stenosis of the proximal RCA (95% with evidence of plaque rupture) is the culprit for the patient's inferoposterior STEMI.
She had this ECG recorded: Obvious massive anterior STEMI She was quickly brought to the criticalcare area and the cath lab was activated. The blood pressure was 170/100 in the criticalcare area. This was ruptured plaque with thrombus. She has no SOB and no prior medical history. Her initial BP was 203/124.
In my review of the literature, there are many articles which purport to demonstrate an acutely increased risk of plaque rupture from emotional stress, but I could not find any credible case reports that were not at least as likely to be takotsubo. Mechanisms of plaque formation and rupture. Coronary plaque disruption.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.













Let's personalize your content