This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Criticalcare cardiology refers to the practice focus of and subspecialty training for the comprehensive management of life-threatening cardiovascular diseases and comorbid conditions that require advanced criticalcare in an intensive care unit. Circulation, Ahead of Print.
Admissions to CICUs with the highest tertile of CCRx utilization had a greater burden of comorbidities, had more diagnoses of ST–elevation myocardialinfarction, cardiac arrest, or cardiogenic shock, and had higher Sequential Organ Failure Assessment scores. CCRx was provided to 62.2% (interhospital range of 21.3%–87.1%)
It turns out that the conventional algorithm was also worried, and because of that, the patient was brought to the criticalcare area. No Previous ECGs Available.
In 1999, Hébert and colleagues published their findings from the landmark Transfusion Requirements in CriticalCare. It is also one of the most overused medical procedures, which largely neglects the associated risks, costs, and sustainability of liberal transfusion practices.
Timing of revascularization in patients with transient ST segment elevation myocardialinfarction: a randomized clinical trial. A comparison of electrocardiographic changes during reperfusion of acute myocardialinfarction by thrombolysis or percutaneous transluminal coronary angioplasty. Lemkes et al. Eur Heart J 2018.
In May 2024, Community Medical Center, a primary stroke center in New Jersey, introduced a protocol to place criticalcare transport vehicles and/or a helicopter on standby when p[2] hysicians and paramedics identified a patient with stroke symptoms, an NIHSS >6 and a RACE score of >5.
The patient was moved to the criticalcare area (stabilization room). Angiogram Culprit Lesion (s): ST elevation myocardialinfarction due to 99% stenosis of the distal LAD Formal echo: Normal estimated left ventricular ejection fraction, 63%. Cath lab was activated. A 2nd ECG recorded 50 minutes after the first.
Alternatively , it is someone who has an old myocardialinfarction and is now very sick with something else. Today’s patient developed the series of 4 tachyarrhythmias shown above in the criticalcare area of the ED. Below is my response. There is sinus tach. There is an incomplete RBBB and LAFB.
Submitted and written by Alex Bracey, with edits by Pendell Meyers and Steve Smith: I was walking through the criticalcare section of the ED when I overheard a discussion about the following ECG. I had no history on the case and no prior ECG for comparison. What do you think? The initial ECG was taken at 0839.
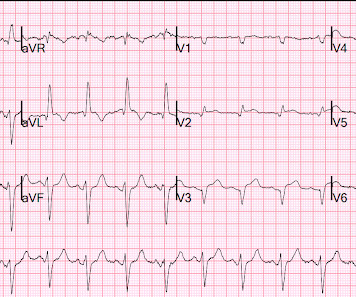
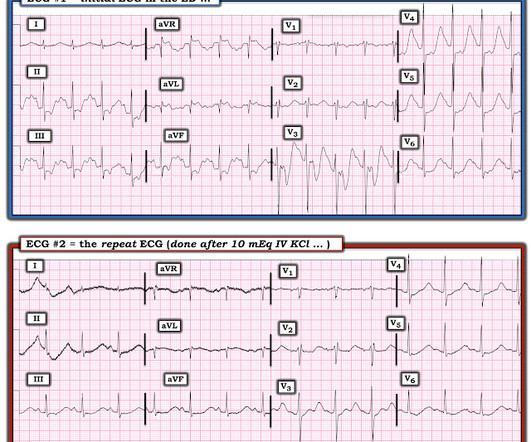
He was moved to the criticalcare area due to his EKG. This was not a myocardialinfarction of any kind. The patient had come to the ED for SOB, but without any chest pain. He has 3 weeks of progressive fatigue and weakness. He had a 10 pound weight loss. His potassium returned at 1.3 Learning Points: 1.
There was high suspicion of OMI, so patient was brought to criticalcare area and another ECG was recorded just 7 minutes later as the pain had diminished to 4/10. Comparison of the ST-Elevation MyocardialInfarction (STEMI) vs. NSTEMI and Occlusion MI (OMI) vs. NOMI Paradigms of Acute MI. 2022.08.750 Section 5.2.2,
We brought the patient into one of our criticalcare rooms and immediately got more history while recording this repeat ECG: The STE in I has greatly diminished or entirely disappeared. Acute myocardialinfarction due to left circumflex artery occlusion and significance of ST-segment elevation. From AM et al.
Crit Care Med. 1991 May;19(5):694-9 Objective: To evaluate the efficacy and safety of potassium replacement infusions in critically ill patients. Setting: Multidisciplinary criticalcare unit. Literature on Hypokalemia as a risk for ventricular fibrillation in acute myocardialinfarction.
The patient arrived at the Emergency Dept criticalcare area and had this ECG recorded: The sinus bradycardia persists. Posterior wall involvement attenuates predictive value of ST-segment elevation in lead V4R for right ventricular involvement in inferior acute myocardialinfarction.
Scott Rankin The Impact of Mitral Disease Etiology on Operative Mortality After Mitral Valve Operations The Annals of Thoracic Surgery November 2018 Alice Wang Robotic Mitral Valve Repair in Older Individuals: An Analysis of The Society of Thoracic Surgeons Database The Annals of Thoracic Surgery November 2018 Mohamad Alaeddine Aortic clamping strategy (..)
Scott Rankin The Impact of Mitral Disease Etiology on Operative Mortality After Mitral Valve Operations The Annals of Thoracic Surgery November 2018 Alice Wang 1 Robotic Mitral Valve Repair in Older Individuals: An Analysis of The Society of Thoracic Surgeons Database The Annals of Thoracic Surgery November 2018 Mohamad Alaeddine 1 Aortic clamping (..)
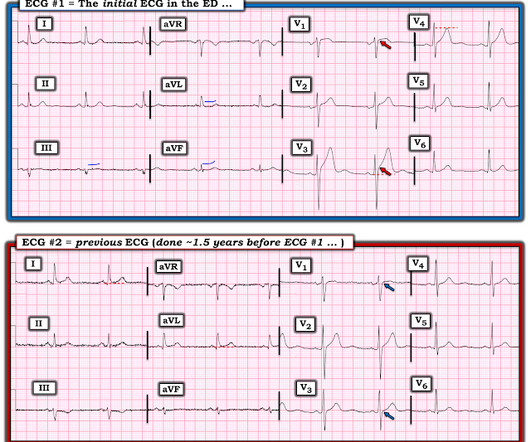
Below are his presenting STEMI ECG and his post-PCI ECG from 3 weeks prior: Because of the hypotension, chest pain, and T-wave inversions, the physicians were worried about MI, took the patient to the criticalcare room, and called the cardiologists. However, these T-wave inversions should be expected at one month after MI.
She had this ECG recorded: Obvious massive anterior STEMI She was quickly brought to the criticalcare area and the cath lab was activated. The blood pressure was 170/100 in the criticalcare area. She has no SOB and no prior medical history. Her initial BP was 203/124. Some Literature 1.3% Acta Cardiol. 2016;32:265272.
The authors describe a case with some features in common with our patient -- a stressful event followed by a stress cardiomyopathy/acute myocardialinfarction overlap syndrome. Acute myocardialinfarction: an uncommon complication of takotsubo cardiomyopathy. Acute myocardialinfarction triggered by emotional stress.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
























Let's personalize your content