This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
It turns out that the conventional algorithm was also worried, and because of that, the patient was brought to the criticalcare area. There is akinesis of the distal septum, anterior, apex, and distal inferior wall consistent with LAD territory ischemia or infarction. How large is the infarct?
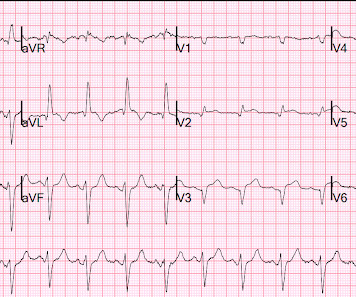
He was rushed by residents into our criticalcare room with a diagnosis of STEMI, and they handed me this ECG: There is sinus tachycardia with ST elevation in II, III, and aVF, as well as V4-V6. He presented to the Emergency Department with a blood pressure of 111/66 and a pulse of 117. He had this ECG recorded.
Perhaps they indicate an open artery with minimal flow and severe subendocardial ischemia, but not total subepicardial ischemia. A male in his 30's complained of sudden severe substernal chest pain. I have often wondered if de Winter's T-waves really are due to complete occlusion, or to severe, subtotal occlusion.
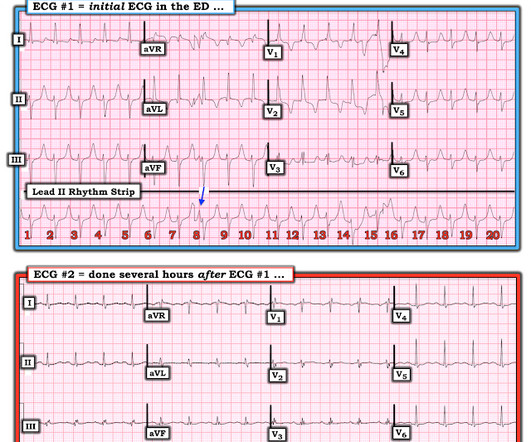
Submitted and written by Alex Bracey, with edits by Pendell Meyers and Steve Smith: I was walking through the criticalcare section of the ED when I overheard a discussion about the following ECG. I had no history on the case and no prior ECG for comparison. What do you think? The initial ECG was taken at 0839.
If you put the inferior and posterior findings together, it is diagnostic of OMI This was read as "inferior ischemia" without any other information by Dr. Richard Gray and as probable reperfused inferior-posterior OMI much later by both me and Pendell Meyers, also without any clinical information.
Her initial troponin I, part of a criticalcare order set, returned at 0.55 Either could be a result of myocardial contusion There is some minimal ST depression -- this could represent ischemia What else is there that could use therapy immediately? ng/mL, and an ECG was recorded: There are no P-waves visible.
This EKG was recorded as part of a standing order for criticalcare. 2 days later This is a typical LVH pattern, without ischemia Patient underwent 4 vessel CABG. He had been smoking an opiate and suddenly collapsed. He was ventilated with BVM on arrival. He awoke with naloxone. He denied any CP or SOB.
We brought the patient into one of our criticalcare rooms and immediately got more history while recording this repeat ECG: The STE in I has greatly diminished or entirely disappeared. Let's zoom in on I and aVL: Lead I (top panel) has less than 1mm of STE. aVL is also less dramatic but still abnormal.
This was interpreted by the treating clinicians as not showing any evidence of ischemia. Given the presentation, the cardiologist stented the vessel and the patient returned to the ICU for ongoing criticalcare. He was intubated in the field and sedated upon arrival at the hospital. Two subsequent troponins were down trending.
Session 510) To Treat or Not to Treat Anatomy and Ischemia? Session 508) Battle of the Imagers - Jeopardy Edition! Session 509) Who Wants to Be a Millionaire in Eradicating Vascular Medicine Disparities?
RCA ischemia often results in sinus bradycardia from vagal reflex or ischemia of the sinus node. The patient arrived at the Emergency Dept criticalcare area and had this ECG recorded: The sinus bradycardia persists. But RV systolic pressure is low, so the RV perfuses during BOTH systole and diastole.
If there is polymorphic VT with a long QT on the baseline ECG, then generally we call that Torsades, but Non-Torsades Polymorphic VT can result from ischemia alone. I have read articles that say that patients without ischemia are at low risk of complications from hypokalemia, But it is not entirely without risk. Crit Care Med.
It is critically important for all EM and criticalcare providers to have an intimate understanding of hyperkalemia and its ECG findings. These include ( among others ) — acute febrile illness — variations in autonomic tone — hypothermia — ischemia/infarction/cardiac arrest — and Hyperkalemia.
The patient might be having cardiac ischemia, but if he is, it is unstable angina or non-STEMI, or perhaps he has not YET pseudonormalized, so serial ECGs may be important. The small amount of ST elevation is persistent, not acute. Acute STEMI would have upright T-waves. This is normal for these patients.
She had this ECG recorded: Obvious massive anterior STEMI She was quickly brought to the criticalcare area and the cath lab was activated. The blood pressure was 170/100 in the criticalcare area. Most dissections which cause coronary ischemia are into the RCA ostium ("ostium" = locations of takeoff of the vessel).
Compared to TTE from 7/3/24: the anterior regional wall motion abnormality is new and is consistent with ischemia/infarction in the LAD territory == MY Comment , by K EN G RAUER, MD ( 11/20 /2024 ): == There are several insightful aspects of today's case. There is STE in V5-6. There are new Q-waves in aVL, V5-6.
It is possible there is microvascular dysfunction producing residual transmural ischemia. But this is most common when there is prolonged ischemia, and this patient had the fastest reperfusion imaginable! Multidisciplinary criticalcare management of electrical storm. link] Jentzer, J. Noseworthy, P. Kashou, A.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






















Let's personalize your content