This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The software generates accurate reports in minutes using inexpensive devices, enabling emergency medicine, criticalcare, internal medicine, hospitalists and primary care physicians to make informed care decisions at the bedside. James Hillis, MBBS, DPhil, director of Clinical Operations at Mass General Brigham AI.
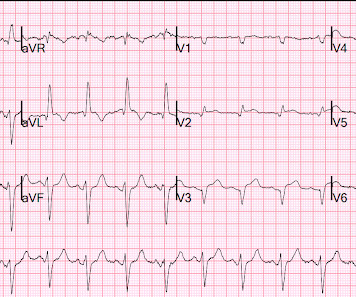
It turns out that the conventional algorithm was also worried, and because of that, the patient was brought to the criticalcare area. The STE in V1 is out of proportion to the S-wave, so V1 is also very worrisome (something I did not see on my phone). So we don't have a good idea how large the final infarct size was.
First troponin I returns at 48 ng/L ECG 5 143 min No significant change ECG 6 261 min Same hs Troponin I profile (peaked at 1849): Formal Echocardiogram SUMMARY The estimated left ventricular ejection fraction is 74 %. Eur Heart J 2018. Full text link. The estimated pulmonary artery systolic pressure is 27 mmHg + RA pressure.
Colin is an emergency medicine resident beginning his criticalcare fellowship in the summer with a strong interest in the role of ECG in criticalcare and OMI. Written by Colin Jenkins. Edits by Willy Frick. This confirms the suspicion of prior anterior OMI. The thrombus is circled below in red.
A 3rd troponin returned before the angiogram was done and was 2956 ng/L Here is the angiogram description: The distal RCA has mild diffuse disease and bifurcates to give a large RPDA which is without significant stenosis. Plus he did a 2 year combined EM Cardiology and CriticalCare Fellowship.
This EKG was recorded as part of a standing order for criticalcare. After discussing all of the above with ED staff, we have made a decision to get stat echocardiogram and assess overall LV function and wall motion abnormalities and defer cath lab activation at the time." He had been smoking an opiate and suddenly collapsed.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












Let's personalize your content