This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
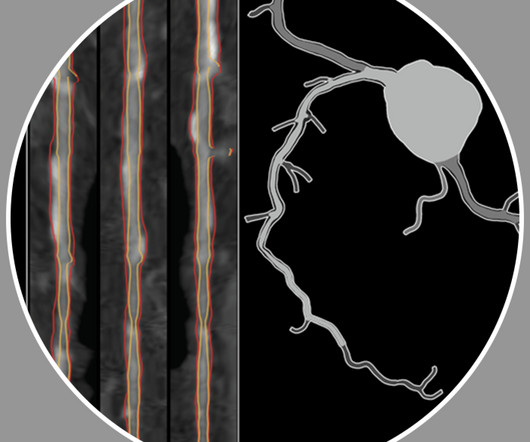
a leader in non-invasive artificial intelligence (AI) heart care solutions, introduced the next generation HeartFlow Plaque Analysis with an interactive experience. Having access to a patient’s whole coronary picture, with both quantified plaque and physiology, is a game changer as a clinician. F.A.C.C.
Reversing or regressing coronaryarterydisease is possible. You cannot eliminate the plaque entirely, but multiple clinical trials have shown plaque regression using high-intensity cholesterol-lowering treatments, which I have discussed previously. REVERSAL Investigators. 2004 Mar 3;291(9):1071-80.
BackgroundPlaque progression (PP) is critical between subclinical atherosclerosis and plaque rupture. After multivariate adjustment, every 0.1mmol/L increase in timeaveraged sdLDLC conferred a 1.2fold increased risk of PP.ConclusionsOur findings suggest that sdLDLC is an independent risk factor of PP in patients with coronaryarterydisease.
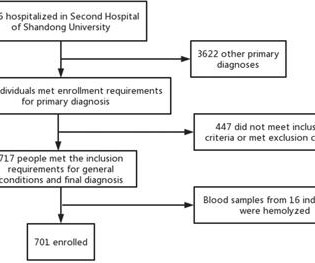
Background To investigate the correlation between lg (circSCMH1/miR-874) and acute coronary syndrome (ACS), acute myocardial infarction (AMI), and carotid plaque stability. Methods 701 patients were divided into stable coronaryarterydisease (SCAD), ACS, and control groups.
Background:Lipoprotein a (Lp(a)) is known to be associated with coronaryarterydisease and carotid artery atherosclerosis. Carotid ultrasound results were divided into two groups based on the presence or absence of plaque. Stroke, Volume 55, Issue Suppl_1 , Page ATP226-ATP226, February 1, 2024.
Angiogram No obstructive epicardial coronaryarterydisease Cannot exclude non-ACS causes of troponin elevation including coronary vasospasm, stress cardiomyopathy, microvascular disease, etc. hours All Hyperacute T-wave and ST Depression is resolved. Echo The estimated left ventricular ejection fraction is 56 %.
Myocardial infarction with non-obstructive coronaryarteries (MINOCA) defines a heterogeneous group of atherosclerotic and non-atherosclerotic conditions, causing myocardial injury in the absence of obstructive coronaryarterydisease.
If the arrest was caused by acute MI due to plaque rupture, then the diagnosis is MINOCA. MINOCA: Myocardial Infarction in the Absence of Obstructive CoronaryArteryDisease). Here is my comment on MINOCA: "Non-obstructive coronarydisease" does not necessarily imply "no plaque rupture with thrombus."
You can easily imagine this patient getting one of several diagnoses -- vasospasm, MINOCA , pericarditis, or maybe even no diagnosis at all beyond "non-obstructive coronaryarterydisease." Smith comment : a very high proportion of MINOCA are ruptured plaque with lysed thrombus. Most plaque is outside the lumen!!
This case was provided by Spencer Schwartz, an outstanding paramedic at Hennepin EMS who is on Hennepin EMS's specialized "P3" team, a team that receives extra training in advanced procedures such as RSI, thoracostomy, vasopressors, and prehospital ultrasound. An angiogram is a "lumenogram;" most plaque is EXTRALUMINAL!!
On arrival, lung ultrasound confirmed pulmonary edema (B lines). Mild Plaque no angiographically significant obstructive coronaryarterydisease. There is STE and hyperacute T-waves in V2 and V3, with significant STE in I and aVL, and inferior reciprocal STD. This is proximal LAD Occlusion until proven otherwise.
Diffuse ST depression with ST elevation in aVR: Is this pattern specific for global ischemia due to left main coronaryarterydisease? Incidence of an acute coronary occlusion. Diffuse ST depression with ST elevation in aVR: Is this pattern specific for global ischemia due to left main coronaryarterydisease?
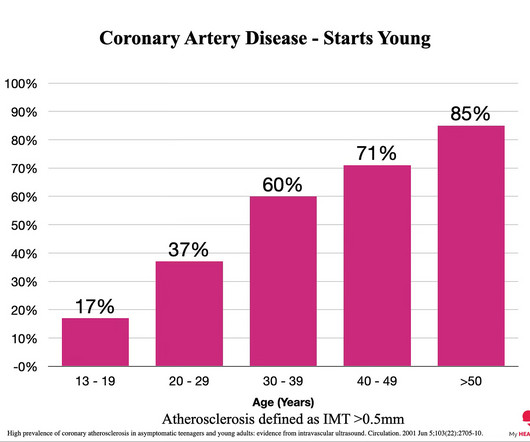
Everyone starts with no plaque in the coronaryarteries, but over a long enough time frame, everyone develops plaque in their coronaryarteries. By age 80, almost everyone will have evidence of advanced plaque in their coronaryarteries, as defined by a cardiac CT 1.
Stone, MD Mount Sinai Health System tim.hodson Wed, 04/02/2025 - 15:26 March 31, 2025 Using intravascular imaging (IVI) to guide stent implantation during complex stenting procedures is safer and more effective for patients with severely calcified coronaryarterydisease than conventional angiography, the more commonly used technique.
BackgroundStudies in young patients with stroke identified coronaryarterydisease (CAD) as a main contributor to mortality. In patients without previous CAD, but femoral plaque on ultrasound, nearly a half had nonobstructive and onefourth had obstructive CAD. During a median followup of 10.1
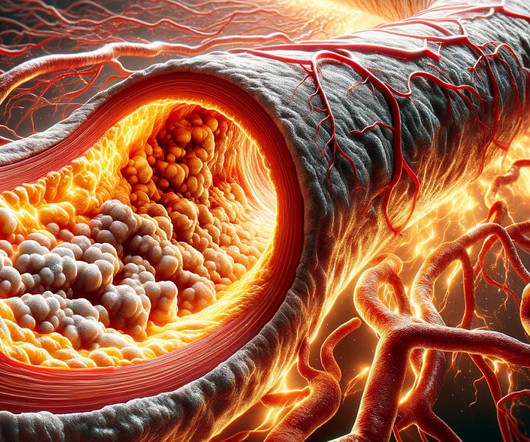
Echocardiography – We can use ultrasound to visualize the heart and look at how well it pumps. With time, fat and cholesterol can get trapped in the areas of wear and tear and cause plaque formation. The plaques can damage us in 2 ways. This is termed as diastolic dysfunction.
The mistake most people make when it comes to heart disease is thinking that when someone has a heart attack that, the condition of ‘heart disease’ just appeared. But heart disease presents slowly. CT Coronary Angiogram. CT Coronary Angiogram. The more plaque, the higher the risk.
Background:The presence of carotid plaque (CP) may serve as an indicator of panvascular atherosclerosis. However, the observed incongruity between carotid disease and the presence and severity of coronaryarterydisease (CAD) suggests differing mechanisms. Subsequently, patients were followed for 5.5
The clinical presentation of ischaemic heart disease has a broad spectrum, encompassing not only traditional epicardial coronaryarterydisease (CAD) characterised by stenosis or occlusion but also structural and functional disorders at both macrovessel and microvessel levels, as highlighted in the latest European guidelines.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




















Let's personalize your content