This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
(MedPage Today) -- ATLANTA -- Fractional flow reserve (FFR)-guided complete revascularization in patients with ST-segment elevation myocardial infarction (STEMI) and multivessel coronaryarterydisease did not result in better outcomes compared.
Later it was shown that index of microvascular resistance which quantified the inability of microcirculation to vasodilate and improve coronary flow after primary PCI, was associated with worst outcomes independent of epicardial coronary flow. Immediate Microvascular Physiology After Mechanical Coronary Reperfusion of STEMI.
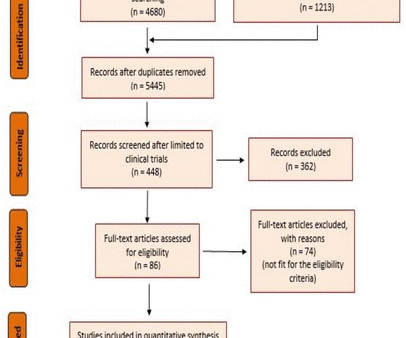
A meta-analysis was performed on primary outcomes of major adverse cardiac events (MACE) and all-cause mortality. A random-effects model was used for outcomes with high heterogeneity.Results:We included 4 RCTs with 3173 patients comparing FFR-guided CR with culprit-only PCI in patients with STEMI and multivessel coronaryarterydiseases.
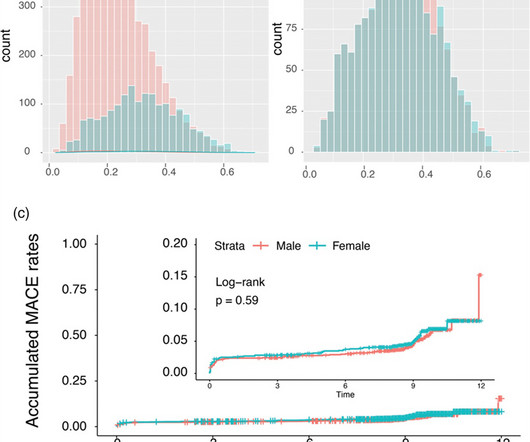
Background: Gender-specific outcomes after percutaneous coronary interventions were studied by a number of research groups with different endpoints and cohorts of different ethnic extractions. In the unmatched STEMI subgroup, all-cause mortality was significantly higher in females driven by older age (P < 0.001).
Old ‘NSTEMI’ A history of coronaryarterydisease and a stent to the same territory further increases pre-test likelihood of acute coronary occlusion, including in-stent thrombosis. So this NSTEMI was likely a STEMI(-)OMI with delayed reperfusion. Deutch et al.
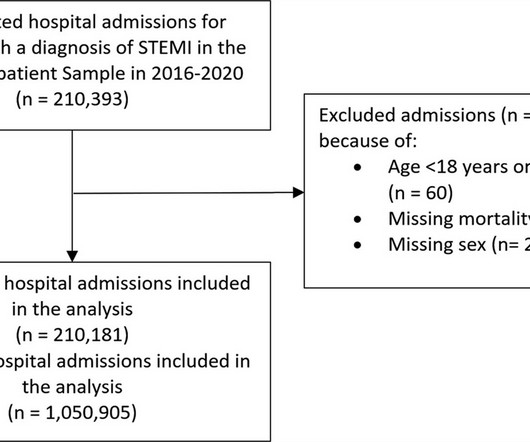
Background It is unclear how COVID-19 pandemic affected care and outcomes among patients who are diagnosed with ST-elevation myocardial infarction (STEMI) in the USA. Results There were 1 050 905 hospitalizations with STEMI, and there was an 8.2% Results There were 1 050 905 hospitalizations with STEMI, and there was an 8.2%
Background Several studies have demonstrated that complete revascularisation improves clinical outcomes in patients with ST-segment elevation myocardial infarction (STEMI) and multivessel coronarydisease. However, the optimal timing of non-culprit lesion revascularisation remains controversial.
Angiogram No obstructive epicardial coronaryarterydisease Cannot exclude non-ACS causes of troponin elevation including coronary vasospasm, stress cardiomyopathy, microvascular disease, etc. Registry data indicate that 6–11% of patients with acute MI have nonobstructive coronaryarteries.
Background Despite improvements in outcomes of ST elevation myocardial infarction (STEMI), ventricular septal rupture (VSR) remains a known complication, carrying high mortality. The contemporary incidence, mortality, and management of post-STEMI VSR remains unclear.
We present the cumulative percutaneous coronary intervention (PCI) data of all comers (stable angina and acute coronary syndromes [ACS]) who presented to Hadi Clinic between January 2018 and December 2020. Prospectively collected data of all comers for PCI (urgent and elective) were retrospectively analysed.
More past history: hypertension, tobacco use, coronaryarterydisease with two vessel PCI to the right coronaryartery and circumflex artery several years prior. He reports that this chest pain feels different than prior chest pain when he had his STEMI/OMI, but is unable to further describe chest pain.
Background Despite advances in percutaneous coronary intervention (PCI) for ST segment elevation myocardial infarction (STEMI), in-hospital mortality remains a concern, highlighting the need for the identification of additional risk factors such as serum iron levels. μmol/L) and a control group (Fe ≥7.8 μmol/L).
Aim Acute injury and subsequent remodelling responses to ST-segment elevation myocardial infarction (STEMI) are major determinants of clinical outcome. Methods and results miRs were quantified in blood samples obtained from patients after primary PCI (PPCI) for STEMI.
Introduction:Inflammation plays an important role in the pathogenesis of coronaryarterydisease and Acute Coronary Syndrome (ACS). Inflammatory indicators such as neutrophil count and monocyte count potentially may predict patients’ outcomes and prognosis in ACS.
This is technically a STEMI, with 1.5 However, I think many practitioners might not see this as a clear STEMI, and would instead call this "borderline." They collected several repeat ECGs at the outside hospital before transport: None of these three ECGs meet STEMI criteria. This ECG was recorded on arrival: What do you think?
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. aVR ST segment elevation: acute STEMI or not? Incidence of an acute coronary occlusion.
Prehospital Conventional algorithm interpretation: ANTERIOR INFARCT, STEMI Transformed ECG by PM Cardio: PM Cardio AI Bot interpretation: OMI with High Confidence What do you think? Mild Plaque no angiographically significant obstructive coronaryarterydisease. She had acute pulmonary edema on exam.
Here is the post shock ECG: Cardiology was called stat for ischemic VT, query SCAD vs thrombotic occlusion vs coronary vasospasm. Cath lab was activated: There was no coronaryarterydisease, but there was spontaneous coronaryartery dissection (SCAD) of the distal LAD, which was narrowed by 95%, and treated medically.
He denied any known medical history, specifically: coronaryarterydisease, hypertension, dyslipidemia, diabetes, heart failure, myocardial infarction, or any prior PCI/stent. It doesn’t meet any conventional STEMI criteria, but there is patently obvious increased area under the curve. No appreciable skin pallor.
A 56 year old male with a history of diabetes, dyslipidemia, hypertension, and coronaryarterydisease presented to the emergency department with sudden onset weakness, fatigue, lethargy, and confusion. At 2111, the troponin I peaked at 12.252 ng/mL (this is in the range of STEMI patients, quite high).
Hospital Course The patient was taken emergently to the cath lab which did not reveal any significant coronaryarterydisease, but she was noted to have reduced EF consistent with Takotsubo cardiomyopathy. Registry data indicate that 6–11% of patients with acute MI have nonobstructive coronaryarteries.
The patient was in his 50s with history of hypertension, diabetes, seizure disorder, and smoking, but no known coronaryarterydisease. He wrote in his note that "The EKG showed early repolarization in I, V2-V3 but no clear STEMI pattern." 418 of these 1788 (23%) had acute coronary occlusion.
When total LM occlusion does present with STE in aVR, there is ALWAYS ST Elevation elsewhere which makes STEMI obvious; in other words, STE is never limited to only aVR but instead it is part of a massive and usually obvious STEMI. All are, however, clearly massive STEMI. This is her ECG: An obvious STEMI, but which artery?
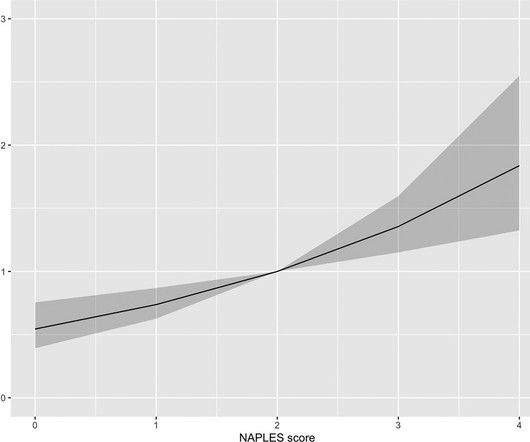
However, the prognostic significance of NPS is unknown in ST-segment elevation myocardial infarction (STEMI). We aimed to analyze the prognostic value of the NPS in-hospital mortality in patients with STEMI. Methods The study consisted of 3828 patients diagnosed with STEMI who underwent primer percutaneous coronary intervention.
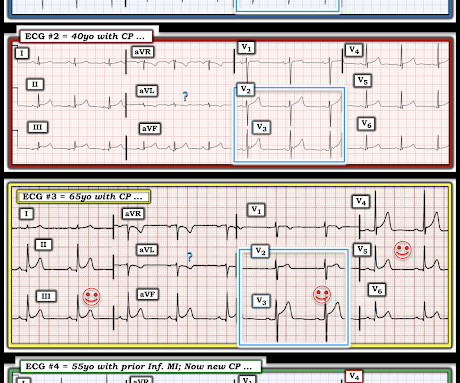
Written by Jesse McLaren, with edits from Meyers Four patients presented with chest pain or shortness of breath, and ECGs labeled ‘inferior STEMI’. Less concavity associated with hyperacuity This can help identify false negative STEMI, or STEMI(-)OMI, at risk for delayed reperfusion. More asymmetry 3.
He has a history of coronaryarterydisease and a STEMI two years prior that was treated with primary PCI. At the time of this initial ED ECG, his symptoms were improving ECG #1 on admission to the ED The patient was not seen quickly in the ED as it was a busy shift and the ECG did not meet STEMI criteria.
Supply-demand mismatch can cause ST Elevation (Type 2 STEMI). Also see these posts of Type II STEMI. An EKG from a year prior was available for comparison: The ED physician noted Initial EKG here read by the computer as a STEMI, however, there is a very poor baseline and a lot of artifact. See reference and discussion below.
Was her outcome to be expected for ostial RCA OMI? Circumstances attending 100 sudden deaths from coronaryarterydisease with coroners necropsies. Frick the ongoing ECG changes in association with hemodynamic collapse seemed out of proportion to the apparent coronary pathology. We will never know for certain.
Introduction The impact of sex on coronaryarterydisease prognosis is debated. We aim to investigate the influence of sex on the timing and clinical outcomes of ST-segment elevation myocardial infarction (STEMI) patients using a controlled Swiss registry. Trial registration number NCT04185285.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





























Let's personalize your content