This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
(MedPage Today) -- ATLANTA -- Fractional flow reserve (FFR)-guided complete revascularization in patients with ST-segment elevation myocardialinfarction (STEMI) and multivessel coronaryarterydisease did not result in better outcomes compared.
Patients with ST-segment elevation myocardialinfarction (STEMI) and complex coronaryarterydisease (CAD) face a poor prognosis, including increased heart failure (HF) risk. We performed a pooled secondary analysis of 139 patients with STEMI.
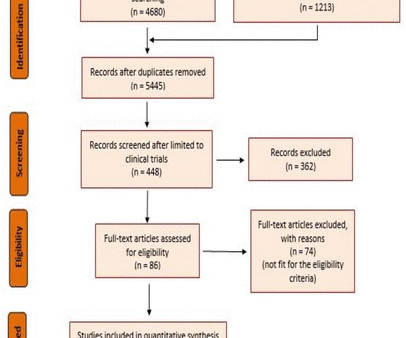
A random-effects model was used for outcomes with high heterogeneity.Results:We included 4 RCTs with 3173 patients comparing FFR-guided CR with culprit-only PCI in patients with STEMI and multivessel coronaryarterydiseases. The pooled results of the 4 RCTs showed that MACE (RR=0.66; 95% CI [0.45, 0.99]; p=0.01; 16.8%
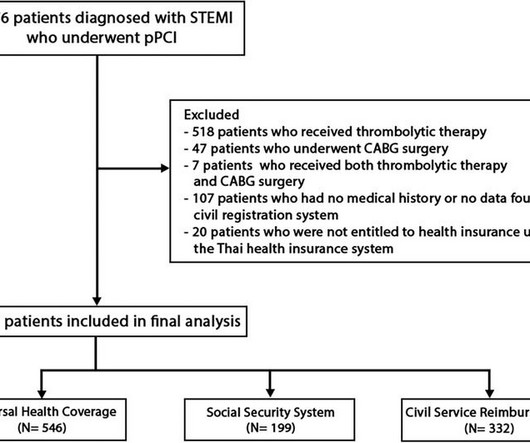
BackgroundIn Thailand, access to specific pharmaceuticals and medical devices for ST-elevation myocardialinfarction (STEMI) patients is restricted within certain healthcare systems, leading to inequalities in the quality of medical care among different healthcare systems.
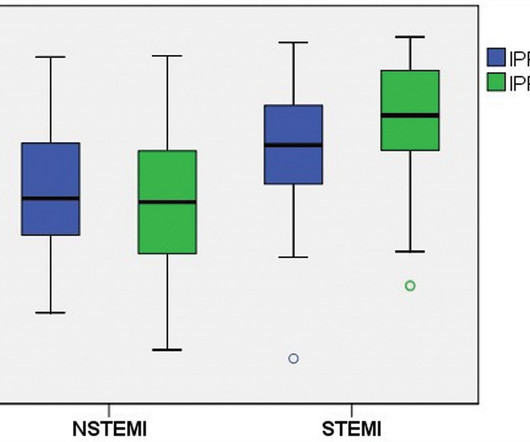
Introduction Elevated peak cardiac troponin levels have been linked with increased morbidity and mortality in patients with acute myocardialinfarction (AMI). Results Among the 277 patients diagnosed with AMI who underwent IPF testing, 113 had (STEMI) and 164 had (NSTEMI). Notably, among STEMI patients, those with IPF ≥ 4.2%
Background Several studies have demonstrated that complete revascularisation improves clinical outcomes in patients with ST-segment elevation myocardialinfarction (STEMI) and multivessel coronarydisease. However, the optimal timing of non-culprit lesion revascularisation remains controversial.
It is now well known that even if a coronaryartery is opened well after a myocardialinfarction, with good flow in the epicardial coronaryarteries, there could be impaired myocardial perfusion. Immediate Microvascular Physiology After Mechanical Coronary Reperfusion of STEMI.
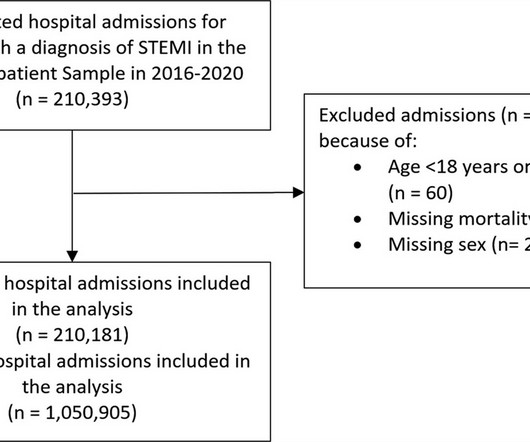
Background It is unclear how COVID-19 pandemic affected care and outcomes among patients who are diagnosed with ST-elevation myocardialinfarction (STEMI) in the USA. Results There were 1 050 905 hospitalizations with STEMI, and there was an 8.2% reduction in admissions in 2020.
Background Despite improvements in outcomes of ST elevation myocardialinfarction (STEMI), ventricular septal rupture (VSR) remains a known complication, carrying high mortality. The contemporary incidence, mortality, and management of post-STEMI VSR remains unclear. and 10 ± 1.2%
In this study, we aimed to investigate the relationship between triglyceride/high-density lipoprotein cholesterol (triglyceride/HDL-C) ratio and SYNTAX scores in patients presenting with non-ST elevation myocardialinfarction (NSTEMI).
Angiogram No obstructive epicardial coronaryarterydisease Cannot exclude non-ACS causes of troponin elevation including coronary vasospasm, stress cardiomyopathy, microvascular disease, etc. In patients presenting with non-ST-segment elevation MI (NSTEMI), the infarct is subendocardial. Lindahl et al.
Purpose Construction of a prediction model to predict the risk of major adverse cardiovascular events (MACE) in the long term after percutaneous coronary intervention (PCI) in patients with acute ST-segment elevation myocardialinfarction (STEMI).
Background Despite advances in percutaneous coronary intervention (PCI) for ST segment elevation myocardialinfarction (STEMI), in-hospital mortality remains a concern, highlighting the need for the identification of additional risk factors such as serum iron levels. μmol/L) and a control group (Fe ≥7.8 μmol/L).
Aim Acute injury and subsequent remodelling responses to ST-segment elevation myocardialinfarction (STEMI) are major determinants of clinical outcome. Current imaging and plasma biomarkers provide delayed readouts of myocardial injury and recovery. A cell culture model was used to identify endothelial cell–derived miRs.
Data were pooled and analyzed in terms of clinical outcomes to assess the impact of gender in patients with stable coronaryarterydisease and acute coronary syndrome. In the unmatched STEMI subgroup, all-cause mortality was significantly higher in females driven by older age (P < 0.001). vs. 5.2%; P = 0.749).
Written by Bobby Nicholson What do you think of this “STEMI”? Second, although there is a lot of ST Elevation which meets STEMI criteria, especially in V3-4, the ST segment is extremely upwardly concave with very large J-waves (J-point notching). With EMS, patient had a GCS of 3 and was saturating 60% on room air. ng/mL and 0.10
Hyperacute T-wave in lead III, with reciprocal findings in aVL -- single lead OMI in the setting of multivessel disease. Aslanger's pattern (Smith was co-author on this): A new electrocardiographic pattern indicating inferior myocardialinfarction The next troponin returned at 8822 ng/L.
When total LM occlusion does present with STE in aVR, there is ALWAYS ST Elevation elsewhere which makes STEMI obvious; in other words, STE is never limited to only aVR but instead it is part of a massive and usually obvious STEMI. All are, however, clearly massive STEMI. This is her ECG: An obvious STEMI, but which artery?
This is technically a STEMI, with 1.5 However, I think many practitioners might not see this as a clear STEMI, and would instead call this "borderline." They collected several repeat ECGs at the outside hospital before transport: None of these three ECGs meet STEMI criteria. This ECG was recorded on arrival: What do you think?
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. aVR ST segment elevation: acute STEMI or not? Incidence of an acute coronary occlusion.
He denied any known medical history, specifically: coronaryarterydisease, hypertension, dyslipidemia, diabetes, heart failure, myocardialinfarction, or any prior PCI/stent. It doesn’t meet any conventional STEMI criteria, but there is patently obvious increased area under the curve. Is this OMI?
Hospital Course The patient was taken emergently to the cath lab which did not reveal any significant coronaryarterydisease, but she was noted to have reduced EF consistent with Takotsubo cardiomyopathy. Such cases are classified as MINOCA (MyocardialInfarction with Non-Obstructed CoronaryArteries).
This is a troponin I level that is almost exclusively seen in STEMI. In this case, profound shock for 1 hour would result in the same degree of infarction. A followup ECG was recorded 2 days later: No definite evidence of infarction. So this is either a case of MINOCA, or a case of Type II STEMI. Troponin I rose to 44.1
Comorbidities included dyslipidaemia 515/567 (90.9%), hypertension 460/567 (81.2%), diabetes 346/567 (61%), known prior coronarydisease 250/567 (44.2%), and smoking 188/567 (33.1%). The radial approach was used in 544/567 (95.94%), the average SYNTAX score was 34.8 ± 9.6, and the average number of stents 2.6.
The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion. Troponin T peaked at 38,398 ng/L ( = a very large myocardialinfarction, but not massive-- thanks to the pre-PCI spontaneous reperfusion, and rapid internvention!! ). The below ECG was recorded. Inotropic medication was continued.
The patient was in his 50s with history of hypertension, diabetes, seizure disorder, and smoking, but no known coronaryarterydisease. He wrote in his note that "The EKG showed early repolarization in I, V2-V3 but no clear STEMI pattern." Of the 418 patient with ACO, 29% did not meet “STEMI criteria.”
See our publication: ST depression in lead aVL differentiates inferior ST-elevation myocardialinfarction from pericarditis There is STE in inferior leads, high lateral leads, and V4-V6. Smith and Meyers to diagnose both obvious (STEMI) and subtle OMI. Result: no angiographically significant obstructive coronaryarterydisease.
ng/mL This single initial troponin at this level, in the context of chest pain, is high enough to be diagnostic of acute myocardialinfarction. A CT Coronary angiogram was ordered. Here are the results: --Minimally obstructive coronaryarterydisease. --LAD It is likely that the artery will re-occlude.
Pseudonormalization of STE and/or STD , as in this patient with LVH, but also in LBBB and other etiologies of chronic ST shift, should raise concern for OMI (Occlusion MyocardialInfarction). If she had no risk factors, it is doubtful that she would have developed such extensive coronaryarterydisease as we see on the angiogram.
Andreas Grüntzig, an ardent angiologist crafted an indeflatable sausage-shaped dual-lumen balloon-catheter, designed its delivery to the heart, launched minimally invasive coronary intervention and taught by beaming live demonstration. Subsequent advances are just incremental tweaks and tinkers around this fully formed framework from 1978.
Clinical Course The paramedic activated a “Code STEMI” alert and transported the patient nearly 50 miles to the closest tertiary medical center. The diagnostic coronary angiogram identified only minimal coronaryarterydisease, but there was a severely calcified, ‘immobile’ aortic valve. What do you see?
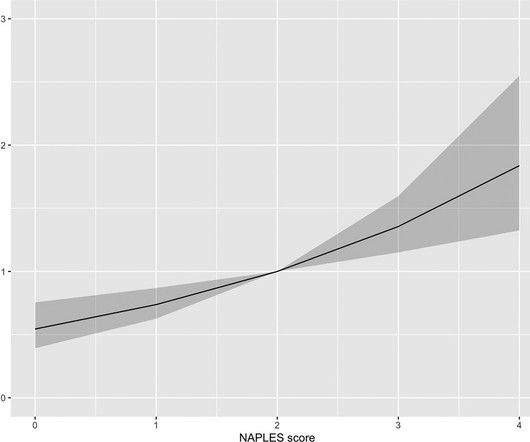
However, the prognostic significance of NPS is unknown in ST-segment elevation myocardialinfarction (STEMI). We aimed to analyze the prognostic value of the NPS in-hospital mortality in patients with STEMI. Conclusion The present study demonstrates that the NPS could independently predict in-hospital mortality in STEMI.
He has a history of coronaryarterydisease and a STEMI two years prior that was treated with primary PCI. At the time of this initial ED ECG, his symptoms were improving ECG #1 on admission to the ED The patient was not seen quickly in the ED as it was a busy shift and the ECG did not meet STEMI criteria.
The authors describe a case with some features in common with our patient -- a stressful event followed by a stress cardiomyopathy/acute myocardialinfarction overlap syndrome. Acute myocardialinfarction: an uncommon complication of takotsubo cardiomyopathy. Coronary plaque disruption. SanzRuiz, R., Solis, J., &
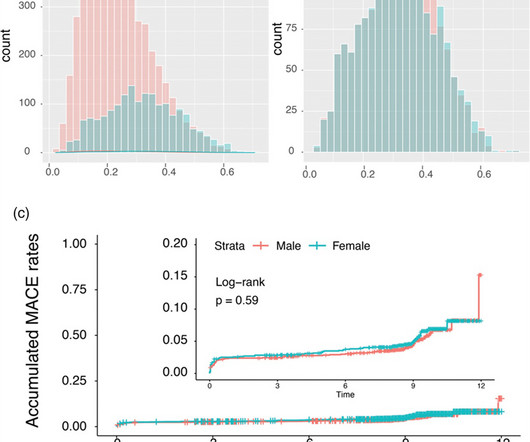
Introduction The impact of sex on coronaryarterydisease prognosis is debated. We aim to investigate the influence of sex on the timing and clinical outcomes of ST-segment elevation myocardialinfarction (STEMI) patients using a controlled Swiss registry.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


































Let's personalize your content