This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
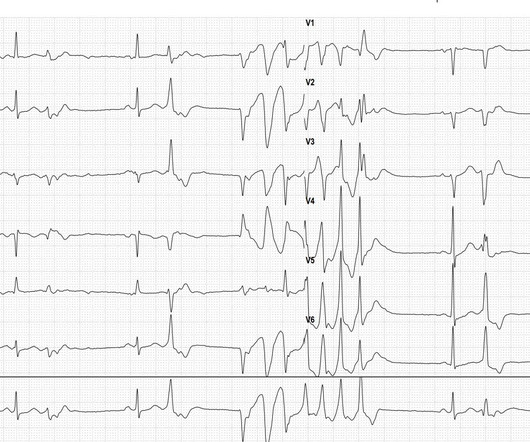
Then, a polymorphic ventricular tachycardia occurs over 7 beats. The QT interval of the sinus beats does not appear prolonged, thus ruling out Torsades de Pointes tachycardia. The most likely cause of this type of polymorphic ventricular tachycardia during a stress EKG is cardiac ischemia/coronaryarterydisease.
Many of the changes seen are reminiscent of LVH with “strain,” and downstream Echo may very well corroborate such a suspicion, but since the ECG isn’t the best tool for definitively establishing the presence of LVH, we must favor a subendocardial ischemia pattern, instead. Type I ischemia. Type II ischemia.
This is ischemic ST depression, and could be due to increasing tachycardia, with a heart rate over 130, but that is unlikely given that the patient is now complaining of crushing chest pain and that there was tachycardia all along. They agreed ischemia was likely in the setting of demand given DKA and infection.
I quickly reviewed the patient’s records and saw that she was a 53 year old woman with a history of BMI 40, but no other identifiable risk factors for coronaryarterydisease. This proves effective treatment of the recurrent ischemia. The patient had no further symptoms of ischemia.
The diagnostic coronary angiogram identified only minimal coronaryarterydisease, but there was a severely calcified, ‘immobile’ aortic valve. DISCUSSION: The 12-lead EKG EMS initially obtained for this patient showed severe ischemia, with profound "infero-lateral" ST depression and reciprocal ST elevation in lead aVR.
His response: “subendocardial ischemia. Smith : It should be noted that, in subendocardial ischemia, in contrast to OMI, absence of wall motion abnormality is common. With the history of Afib, CTA abdomen was ordered to r/o mesenteric ischemia vs ischemic colitis vs small bowel obstruction. Anything more on history?
ECG in a person with persistent anginal pain for the past several hours showing significant ST segment depression anterolateral leads along with sinus tachycardia. Such a pattern is consistent with significant left main coronaryartery stenosis. ST elevation in aVR more than that in V1 is also suggestive of left main disease.
A 56 year old male with a history of diabetes, dyslipidemia, hypertension, and coronaryarterydisease presented to the emergency department with sudden onset weakness, fatigue, lethargy, and confusion. The patient’s angiogram should have been expedited, but the EKG change was not recognized as recurrence of transmural ischemia.
Diffuse ST depression with ST elevation in aVR: Is this pattern specific for global ischemia due to left main coronaryarterydisease? Ischemia b. ST depression: is it ischemia? It was a baseline finding in 62% of patients, usually due to LVH. Reference: Knotts RJ , Wilson JM, Kim E, Huang HD, Birnbaum Y.
These findings are concerning for inferior wall ischemia with possible posterior wall involvement. He was taken emergently to the cardiac catheterization lab and found to have multi-vessel coronaryarterydisease with a near-occlusive culprit lesion in the RCA, possibly reperfused. No significant changes, ongoing pain.
The first task when assessing a wide complex QRS for ischemia is to identify the end of the QRS. The ST segment changes are compatible with severe subendocardial ischemia which can be caused by type I MI from ACS or potentially from type II MI (non-obstructive coronaryarterydisease with supply/demand mismatch).
This progressed to electrical storm , with incessant PolyMorphic Ventricular Tachycardia ( PMVT ) and recurrent episodes of Ventricular Fibrillation ( VFib ). There is no definite evidence of acute ischemia. (ie, If there had been ECG findings indicating reocclusion of the artery — an angiogram would have been warranted ).
A fast heartbeat is called tachycardia, while a slow heartbeat is called bradycardia in medical terms. Poor blood supply Ischemia, or inadequate blood supply to the heart, is an abnormality that can be detected in an ECG test. ECG machine can also help diagnose coronaryarterydisease.
Post by Smith and Meyers Sam Ghali ( [link] ) just asked me (Smith): "Steve, do left main coronaryartery *occlusions* (actual ones with transmural ischemia) have ST Depression or ST Elevation in aVR?" Here I explain: First, you don't know for certain what the state of the artery was at the time of the ECG.
Written by Willy Frick with edits by Ken Grauer An older man with a history of non-ischemic HFrEF s/p CRT and mild coronaryarterydisease presented with chest pain. No evidence for ischemia jumps out. So the most likely rhythm in ECG 1 is ectopic atrial tachycardia. ECG 1 What do you think? Point 1: What is PVARP?
The status of the patients chest pain at this time is unknown : EKG 1, 1300: There is sinus tachycardia and artifact of low and high frequency. However, there is also significant tachycardia , with heart rate of 116, and known hypoxia. The patient was started on heparin for possible NSTEMI vs demand ischemia.
September 2024 Approvals Flurpiridaz F 18 Approval Date: September 27, 2024 Indication: A radioactive positron emission tomography (PET) tracer for imaging myocardial ischemia and infarction in adults with suspected or known coronaryarterydisease. Heart rate reduction within 10 minutes : Landiolol: 40%-90%.
Ventricular tachycardia?) Severe ischemia can be present even when the chest pain is gone. He said it felt like "someone ripped [his] heart out." While walking into the ED, the patient had an episode of "dizziness" causing him to fall onto his stomach. What do you think? I sent this ECG to Dr. Smith and Dr. Meyers with no context.
Written by Pendell Meyers A woman in her 70s with known prior coronaryarterydisease experienced acute chest pain and shortness of breath. One could argue or wonder if there is both subendocardial ischemia AND posterior OMI pattern, since the STD in V4 may be equal or possibly slightly worse proportionally than V6.
It is possible there is microvascular dysfunction producing residual transmural ischemia. But this is most common when there is prolonged ischemia, and this patient had the fastest reperfusion imaginable! Circumstances attending 100 sudden deaths from coronaryarterydisease with coroners necropsies. link] Park, J.,
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



























Let's personalize your content