This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
In the ISCHEMIA (International Study of Comparative Health Effectiveness with Medical and Invasive Approaches) trial, researchers examined the risk of ischemic events in patients with stable coronaryarterydisease. years, with 57.1% occurring within 30 days after CABG. Original article: Redfors B et al.
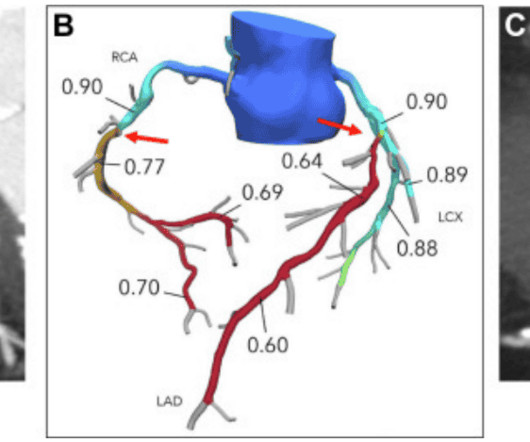
Together, the two companies will work to further the development and commercialization of Medis Quantitative Flow Ratio (Medis QFR), a non-invasive approach to the assessment of coronary physiology, as part of GE HealthCare’s interventional cardiology portfolio built around the Allia Platform.
Hemodynamic reactivity, changes in endothelial function, and vasoconstriction during mental stress were evaluated using changes in ratepressure product, brachial artery flowmediated vasodilation, and peripheral arterial tonometry, respectively. A total of 629 participants were included.
1 Atherosclerosis is a systemic disease that affects multiple vascular regions and is particularly severe in PAD patients, where up to 80 percent suffer from concurrent coronaryarterydisease (CAD), historically linked with a mortality rate exceeding 50 percent within five years.
A study in the Journal of Vascular Surgery revealed that adding FFRCT assessments to patient workups prior to peripheral arterydisease surgeries has a massive impact on coronaryarterydisease detection, treatments, and long-term outcomes.
Background:Myocardial infarction with nonobstructive coronaryarterydisease (MINOCA) is a special syndrome with clear evidence of myocardialischemia, but no clear stenosis of coronaryartery imaging sign. Circulation, Volume 150, Issue Suppl_1 , Page A4143007-A4143007, November 12, 2024.
Important point: when there is diffuse subendocardial ischemia but no OMI, a wall motion abnormality will not necessarily be present. They agreed ischemia was likely in the setting of demand given DKA and infection. That this is all demand ischemia is unlikely. Lung exam showed diffuse B lines bilaterally. Aslanger's pattern.
Background Untreated multivessel disease (MVD) in acute myocardialinfarction (AMI) has been linked to a higher risk of recurrent ischemia and death within one year. The immediate non-IRA PCI is associated with a significantly lower occurrence of unplanned ischemia-driven PCI (OR 0.60; confidence interval [CI] 0.44–0.83)
indicates inducible ischemia while an FFR above 0.80 excludes ischemia in 90% of cases. FAME study showed that at one year follow up, rate of major adverse coronary events was reduced by approximately 30% by routinely measuring FFR. They had lower rates of mortality or myocardialinfarction. Normal FFR is 1.0
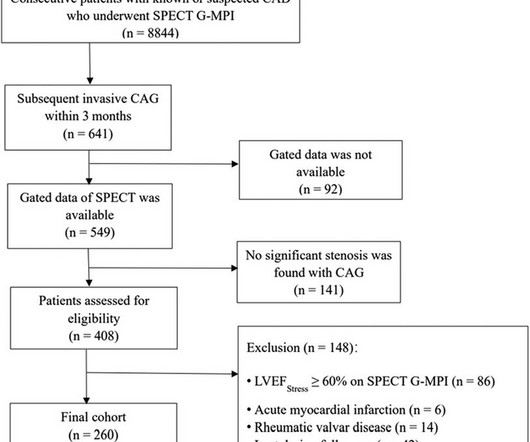
In this study, we aimed to evaluate the prognostic value of ΔLVEF when acquired by SPECT G-MPI in patients with coronaryarterydisease (CAD) and a LVEFStress 0% and ΔLVEF ≤ 0%), and survival analyses were conducted.
Atherosclerotic cardiovascular disease (ASCVD), caused by plaque buildup in arterial walls, is one of the leading causes of disability and death worldwide.1,2 1,2 ASCVD causes or contributes to conditions that include coronaryarterydisease (CAD), cerebrovascular disease, and peripheral vascular disease (inclusive of aortic aneurysm).3
By Magnus Nossen, edits by Grauer and Smith The patient is a 70-something female with DMII, HTN and an extensive prior history of coronaryarterydisease and myocardialinfarctions. ECG#1 Assessing ischemia on an ECG with wide QRS complexes (AIVR, ventricular pacing, BBB, etc) can be challenging.
Angiogram No obstructive epicardial coronaryarterydisease Cannot exclude non-ACS causes of troponin elevation including coronary vasospasm, stress cardiomyopathy, microvascular disease, etc. Detailed coronaryartery evaluation not performed. This suggests further severe ischemia.
The outcome measure was peri-procedural complications defined as a composite of perioperative death, major bleeding, contrast nephropathy, myocardialinfarction, ischemic stroke, and major amputation. A history of coronaryarterydisease was noted in 40.7% Notable comorbidities included diabetes mellitus at 60.6%
The diagnostic coronary angiogram identified only minimal coronaryarterydisease, but there was a severely calcified, ‘immobile’ aortic valve. DISCUSSION: The 12-lead EKG EMS initially obtained for this patient showed severe ischemia, with profound "infero-lateral" ST depression and reciprocal ST elevation in lead aVR.
Post by Smith and Meyers Sam Ghali ( [link] ) just asked me (Smith): "Steve, do left main coronaryartery *occlusions* (actual ones with transmural ischemia) have ST Depression or ST Elevation in aVR?" Here I explain: First, you don't know for certain what the state of the artery was at the time of the ECG.
This highlights the need for serial ECGs in acute coronary syndrome as initial ECGs may be near normal even in those with severe disease. Classical electrocardiographic pattern in left main coronaryarterydisease is ST elevation in aVR with extensive ST depression in other leads, most prominent in I, II and V4-V6.
Troponin T peaked at 38,398 ng/L ( = a very large myocardialinfarction, but not massive-- thanks to the pre-PCI spontaneous reperfusion, and rapid internvention!! ). There is no definite evidence of acute ischemia. (ie, Some residual ischemia in the infarct border might still be present.
Without oxygen, the cells would quickly die, leading to a heart attack (myocardialinfarction). Removal of Deoxygenated Blood via Coronary Veins After the heart muscle cells have extracted oxygen from the blood, the deoxygenated blood needs to be carried away. CAD is one of the leading causes of heart attacks.
CTA head and neck were obtained and showed no evidence of intracranial hemorrhage, large vessel occlusion stroke (what a helpful and apt name for an acute arterial occlusion paradigm, by the way.), or basilar ischemia. Preliminary findings documented in the cath lab were “Anterior STEMI and no significant coronaryarterydisease.” (!!!)
His response: “subendocardial ischemia. Smith : It should be noted that, in subendocardial ischemia, in contrast to OMI, absence of wall motion abnormality is common. With the history of Afib, CTA abdomen was ordered to r/o mesenteric ischemia vs ischemic colitis vs small bowel obstruction. Anything more on history?
CT coronary angiography, in addition to a CT CAC, is arguably the best test for estimating whether someone has evidence of coronaryarterydisease and what that means for their near-term risk of a heart attack. 2 Coronary CT Angiography and 5-Year Risk of MyocardialInfarction. Medicine (Baltimore).
Diamond and Forrester accomplished this by first establishing the prevalence of coronaryarterydisease based on how clinically likely patients with chest pain symptoms were found to have coronarydisease based on a coronary angiogram. Thanks for reading Dr. Anish Koka's Newsletter! This happens.
She requires maximal medical management per all current guidelines (including heparin and P2Y12 inhibitor per cardiology), as well as consideration for emergent cath in the case of persistent ischemia. So what will you do for this patient? They found an acute, total, thrombotic occlusion of the proximal LAD. They opened it. Patel et al.,
Hospital Course The patient was taken emergently to the cath lab which did not reveal any significant coronaryarterydisease, but she was noted to have reduced EF consistent with Takotsubo cardiomyopathy. Such cases are classified as MINOCA (MyocardialInfarction with Non-Obstructed CoronaryArteries).
The highly impactful International Study of Comparative Health Effectiveness With Medical and Invasive Approaches ( ISCHEMIA ) trial investigated the effectiveness of invasive (INV) versus conservative (CON) strategies for managing stable coronaryarterydisease. Original article: Gaudino M et al. EuroIntervention.
In most cases, rather, the culprit is gross ischemia due to myocardialinfarction, cardiomyopathy, or advanced coronaryarterydisease. Unfortunately, today’s case is lacking any such diagnostics, thus I cannot say with certainty that the QT interval is, or is not, culpable in arrhythmogenesis. [1]
The patient was in his 50s with history of hypertension, diabetes, seizure disorder, and smoking, but no known coronaryarterydisease. If the patient had been "lucky," his symptoms from the prior day might have been due to ischemia prolonged and intense enough to result in small troponin increase. From AM et al.
We evaluated the primary outcome (cardiovascular death, myocardialinfarction, or hospitalization for unstable angina, heart failure, or resuscitated cardiac arrest) and other end points, by sex, in 1168 (22.6%) women and 4011 (77.4%) men. Women had less coronaryarterydisease: multivessel in 60.0%
In a study published by the American Heart Association, “Sex and Age Differences in the Association of Depression With Obstructive CoronaryArteryDisease and Adverse Cardiovascular Events,” researchers investigated 3,237 patients (35% women) undergoing coronary angiography to evaluate for coronaryarterydisease (CAD).
HIV and Cardiovascular Disease: HIV infection itself is associated with an increased risk of cardiovascular disease and can double the risk of CVDs, including myocardialinfarction and stroke. Plus, abacavir, an NRTI, has been linked to an increased risk of myocardialinfarction.
He has a history of coronaryarterydisease and a STEMI two years prior that was treated with primary PCI. ECG #3 is easily recognized as OMI and the AI model recommends immediate revascularization The patient in today's case received suboptimal care and suffered a substantial myocardialinfarction. Abstract 556.
Watch what happends as the heart recovers from its episode of ischemia. Angiogram: Severe two-vessel coronaryarterydisease of a left dominant system including 70 to 80% stenosis involving the distal left main/bifurcation. The ECG shows inferior ischemia. Are the T-waves in leads I and II hyperacute? Hard to tell.
It is possible there is microvascular dysfunction producing residual transmural ischemia. But this is most common when there is prolonged ischemia, and this patient had the fastest reperfusion imaginable! Acute myocardialinfarction: an uncommon complication of takotsubo cardiomyopathy. Coronary plaque disruption.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



































Let's personalize your content