This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Old ‘NSTEMI’ A history of coronaryarterydisease and a stent to the same territory further increases pre-test likelihood of acute coronary occlusion, including in-stent thrombosis. So this NSTEMI was likely a STEMI(-)OMI with delayed reperfusion. Deutch et al.
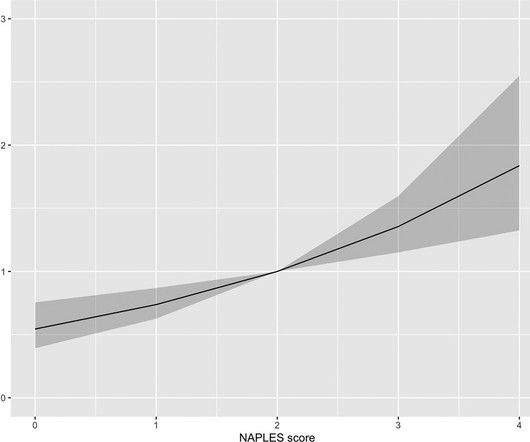
Purpose Construction of a prediction model to predict the risk of major adverse cardiovascular events (MACE) in the long term after percutaneous coronary intervention (PCI) in patients with acute ST-segment elevation myocardial infarction (STEMI).
Case submitted and written by Mazen El-Baba MD, with edits from Jesse McLaren and edits/comments by Smith and Grauer A 90-year old with a past medical history of atrial fibrillation, type-2 diabetes, hypertension, dyslipidemia, presented with acute onset chest/epigastric pain, nausea, and vomiting. Incidence of an acute coronary occlusion.
Vital signs were noted to be unremarkable with respect to any hypo-hypertensive crisis, hypoxia, etc. He denied any known medical history, specifically: coronaryarterydisease, hypertension, dyslipidemia, diabetes, heart failure, myocardial infarction, or any prior PCI/stent. No appreciable skin pallor.
A 56 year old male with a history of diabetes, dyslipidemia, hypertension, and coronaryarterydisease presented to the emergency department with sudden onset weakness, fatigue, lethargy, and confusion. At 2111, the troponin I peaked at 12.252 ng/mL (this is in the range of STEMI patients, quite high).
This patient, who is a mid 60s female with a history of hypertension, hyperlipidemia and GERD, called 911 because of chest pain. A mid 60s woman with history of hypertension, hyperlipidemia, and GERD called 911 for chest pain. An apical OMI has the same ultrasound findings as takotsubo, and thus mimics takotsubo. Lindahl et al.
The patient was in his 50s with history of hypertension, diabetes, seizure disorder, and smoking, but no known coronaryarterydisease. He wrote in his note that "The EKG showed early repolarization in I, V2-V3 but no clear STEMI pattern." 418 of these 1788 (23%) had acute coronary occlusion.
The patient stated he had a long history of well-controlled hypertension for which he was compliant with his ACE-inhibitor. He was taken emergently to the cardiac catheterization lab and found to have multi-vessel coronaryarterydisease with a near-occlusive culprit lesion in the RCA, possibly reperfused.
It was edited by Smith CASE : A 52-year-old male with a past medical history of hypertension and COPD summoned EMS with complaints of chest pain, weakness and nausea. Clinical Course The paramedic activated a “Code STEMI” alert and transported the patient nearly 50 miles to the closest tertiary medical center. What do you see?
Diffuse ST depression with ST elevation in aVR: Is this pattern specific for global ischemia due to left main coronaryarterydisease? Does this patient have hypertension and/or heart failure that has worsened? This might be a common scenario given this patients demographics and his underlying disease ).
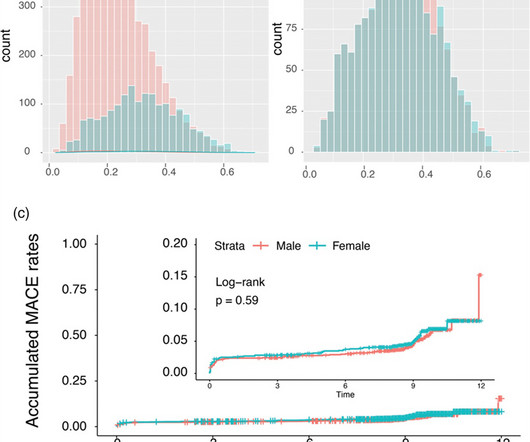
Data were pooled and analyzed in terms of clinical outcomes to assess the impact of gender in patients with stable coronaryarterydisease and acute coronary syndrome. After propensity-score-matching, primarily adjusting for age, hypertension and diabetes, our data revealed similar accumulated MACE in women and men (5.5%
More past history: hypertension, tobacco use, coronaryarterydisease with two vessel PCI to the right coronaryartery and circumflex artery several years prior. Sensitivity was 87% for OMI in our validation study (it was 34% for STEMI criteria). He reports feeling nauseated with emesis.
A middle-aged woman with history of hypertension presented to another hospital approximately 2 hours after onset of chest pain and shortness of breath. This is technically a STEMI, with 1.5 However, I think many practitioners might not see this as a clear STEMI, and would instead call this "borderline." mm STE in V1 and 1.5-2.0
However, the prognostic significance of NPS is unknown in ST-segment elevation myocardial infarction (STEMI). We aimed to analyze the prognostic value of the NPS in-hospital mortality in patients with STEMI. Methods The study consisted of 3828 patients diagnosed with STEMI who underwent primer percutaneous coronary intervention.
Written by Willy Frick A 52 year old man with hypertension, dyslipidemia, and seropositive rheumatoid arthritis (a risk factor for CAD) presented with acute substernal chest pressure with diaphoresis which woke him from sleep just after midnight. He said it felt like "someone ripped [his] heart out." But that is not what happened.
A 69 year old woman with a history of hypertension presented to the emergency department by EMS for evaluation of chest pain and shortness of breath. Supply-demand mismatch can cause ST Elevation (Type 2 STEMI). Also see these posts of Type II STEMI. Truly, the Marquette 12 SL algorithm correctly identifies this STEMI.
Introduction The impact of sex on coronaryarterydisease prognosis is debated. We aim to investigate the influence of sex on the timing and clinical outcomes of ST-segment elevation myocardial infarction (STEMI) patients using a controlled Swiss registry. Disparities are more related to patient characteristics than sex.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.























Let's personalize your content