This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
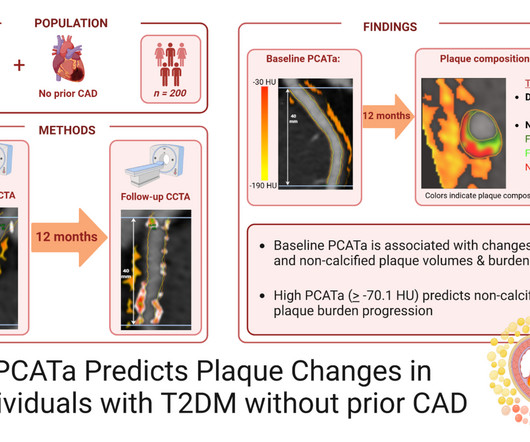
Pericoronary adipose tissue attenuation (PCATa), derived from coronary computed tomography angiography (CCTA), is a novel marker of inflammation in the coronaryarteries. Patients with type 2 diabetes mellitus.
We investigated whether treatment with LDE-paclitaxel changes plaque progression by coronary CT angiography and is safe in patients with chronic coronaryarterydisease. Analysis of inflammatory biomarkers and coronary CTA was also performed at baseline and 4 weeks after treatment.
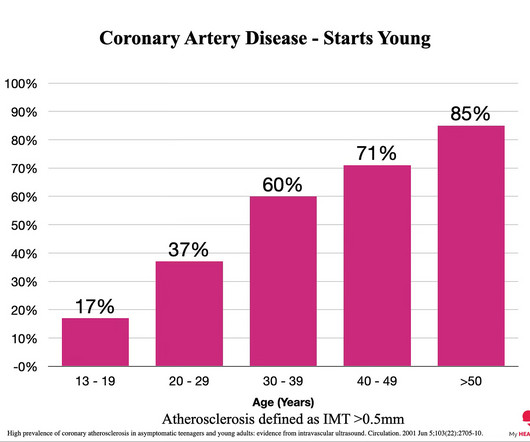
Everyone starts with no plaque in the coronaryarteries, but over a long enough time frame, everyone develops plaque in their coronaryarteries. By age 80, almost everyone will have evidence of advanced plaque in their coronaryarteries, as defined by a cardiac CT 1.
Background In this study, we aim to investigate the relationship between the attenuation of peri-coronary adipose tissue (PCAT) in patients with suspected coronaryarterydisease (CAD) and the assessment of coronary vascular functions using coronary flow reserve (CFR). HU vs. −81.8 HU;
A common feedback I get is that people with existing coronaryarterydisease feel like it doesn’t apply to them. Arguably, applying the principles of prevention offers more bang for buck in the short term for people WITH coronaryarterydisease than those without coronaryarterydisease.
BackgroundPlaque progression (PP) is critical between subclinical atherosclerosis and plaque rupture. P=0.006), especially in diabetic patients (Pearsonr=0.58,P<0.001). Journal of the American Heart Association, Ahead of Print. P<0.001).
Food and Drug Administration ( FDA ) approval for the AGENT Drug-Coated Balloon (DCB), which is indicated to treat coronary in-stent restenosis (ISR) in patients with coronaryarterydisease. ISR is the obstruction or narrowing of a stented vessel by plaque or scar tissue.
Therefore, if someone presents with an event earlier than this age, they likely have been building up plaque for a considerable period prior to this. Here is what I DON’T consider as early heart disease. ” Here is what I DO consider as early heart disease. Most of the time, coronaryarterydisease will be the cause.
To prevent heart disease, you need to know what causes it, how to measure the relevant factors and what to do about them. When we say heart disease, what we really mean is plaque in the artery wall. For every one standard deviation increase of ApoB, the risk of coronaryarterydisease increases by 65% 2.
BACKGROUND:Aortic arch plaques are associated with an increased risk of ischemic stroke in patients with cryptogenic stroke or prior embolic events. Arch plaques were assessed by suprasternal transthoracic echocardiography; plaques ≥4 mm in thickness were classified as large plaques. Stroke, Ahead of Print.
A family history of heart disease often indicates that genetic factors might be at play. Common Heart Diseases with Genetic Links CoronaryArteryDisease (CAD): CAD occurs when the arteries supplying blood to the heart become narrowed or blocked.
BACKGROUND:Individuals with type 2 diabetes (T2D) have an increased risk of coronaryarterydisease (CAD), but questions remain about the underlying pathology. BothATP1B1andARVCFalso had significantly different associations for CAC in T2D cases versus controls.
Atherosclerotic cardiovascular disease (ASCVD), caused by plaque buildup in arterial walls, is one of the leading causes of disability and death worldwide.1,2 7 Research has shown inflammation plays a significant role in the development of atherosclerosis and ASCVD,8-10 and even the formation of plaque.11 4 In the U.S.
Introduction:Since the advent of percutaneous coronary intervention (PCI), the scope of this therapeutic intervention has broadened to include cases of life-threatening multivessel coronaryarterydisease that previously may have only been corrected surgically.
Heart Valve Disease If one or more heart valves are not functioning correctly, it can cause blood to flow backward, putting extra pressure on the heart, which may cause it to expand to compensate for the inefficiency. Monitor cholesterol levels and manage conditions like diabetes that can strain the heart.
PAD is a serious, progressive cardiovascular disease primarily caused by a buildup of fatty plaque in the blood vessels, or atherosclerosis. This plaque narrows the blood vessels and reduces blood flow to the legs and feet, which may significantly impair physical function, walking performance and quality of life.
Giovanna Liuzzo (Italy) revealed that advancements in noninvasive imaging recently allow for direct visualization of coronary atherosclerotic plaques. Dr. Pradeep Natarajan (United States of America) suggested that polygenic risk scores could play a larger role in identifying individuals at risk for cardiovascular disease (CVD).
A heart attack, or myocardial infarction, happens when an artery becomes blocked, reducing blood flow to the heart muscle. This blockage is often caused by a blood clot or the buildup of plaque in the coronaryarteries, which supply the heart with oxygen-rich blood.
STEP-HFpEF DM 5 ( NCT04916470 ) explored the effects of semaglutide in obesity-related HF with preserved ejection fraction (HFpEF) and type 2 diabetes. TACT-2 8 ( NCT02733185 ) assessed if chelation therapy could reduce recurrence of cardiac events in diabetic patients with prior MI.
High cholesterol levels – Elevated levels of bad cholesterol can contribute to plaque buildup in your arteries, increasing the risk of heart disease. Smoking – Smoking is the most preventable cause of heart disease. It damages blood vessels, decreases oxygen to the heart and raises the risk of heart disease.
Written by Magnus Nossen The patient in today's case is a male in his 70s with hypertension and type II diabetes mellitus. The ST segment changes are compatible with severe subendocardial ischemia which can be caused by type I MI from ACS or potentially from type II MI (non-obstructive coronaryarterydisease with supply/demand mismatch).
Case submitted and written by Mazen El-Baba MD, with edits from Jesse McLaren and edits/comments by Smith and Grauer A 90-year old with a past medical history of atrial fibrillation, type-2 diabetes, hypertension, dyslipidemia, presented with acute onset chest/epigastric pain, nausea, and vomiting. Incidence of an acute coronary occlusion.
Brittany Weber, MD, PhD , of Brigham and Women’s Hospital, is the 2024 YIA winner for her abstract, "The Frequency, Prevalence, And Outcomes Of Incidentally Detected CoronaryArtery Calcium Using Artificial Intelligence Analysis Among Patients With Immune Mediated Inflammatory Diseases.”
Background:The presence of carotid plaque (CP) may serve as an indicator of panvascular atherosclerosis. However, the observed incongruity between carotid disease and the presence and severity of coronaryarterydisease (CAD) suggests differing mechanisms. Subsequently, patients were followed for 5.5
Background The relationship between atherosclerosis and endotypes of myocardial ischaemia with no obstructive coronaryarterydisease (INOCA) is unclear. Angiograms were examined for luminal stenosis in each segment of the SYNTAX coronary model. Angiographic analyses were performed blind to coronary physiology findings.
Diabetes and Obesity Care Advancements New Technologies for Diabetes Management : The recent FDA approvals of various insulin delivery devices, including the Embecta patch pump for Type 2 diabetes , have expanded patient options. New developments in continuous glucose monitors (CGMs) have also been transformative.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

























Let's personalize your content