This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Insulin resistance and chronic kidneydisease are both associated with increased coronaryarterydisease risk. Many formulae estimating glucose disposal rate in type 1 diabetes infer insulin sensitivity from c.
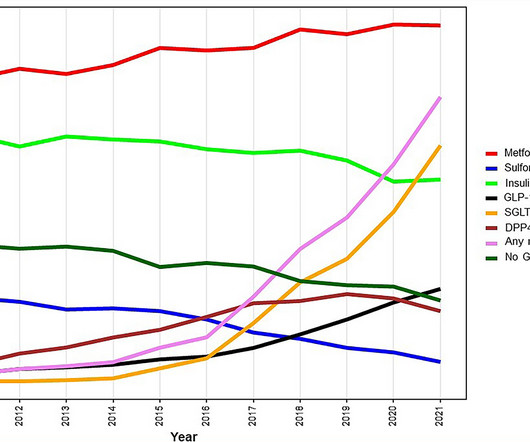
Objective To explore trends in prognosis and use of glucose-lowering drugs (GLD) in patients with diabetes and coronaryarterydisease (CAD). Information on GLD (dispended 6 months before or after coronary angiography) was collected from the Swedish Prescribed Drug Registry. vs. 6.8%), myocardial infarction (7.7%
Methods A cohort of 1245 individuals without chronic kidneydisease from southwest China who underwent coronary angiography between February 2018 and June 2021 were enrolled. CTO was defined as a total occlusion of any coronaryartery or arteries for more than 3 months. 5.89), nonobese individuals (OR, 1.9;
BackgroundThe relation between age at diagnosis of type 2 diabetes (T2D) and hospitalization for heart failure (HHF) is unclear. We identified people with new‐onset T2D between April 1, 2005 and March 31, 2015, and matched each person with 3 diabetes‐free adults, according to birth year and sex. 2.56]) relative to matched individuals.
Atherosclerotic cardiovascular disease (ASCVD), caused by plaque buildup in arterial walls, is one of the leading causes of disability and death worldwide.1,2 1,2 ASCVD causes or contributes to conditions that include coronaryarterydisease (CAD), cerebrovascular disease, and peripheral vascular disease (inclusive of aortic aneurysm).3
Among those ages 65 and older, nearly 50% who underwent limb amputation died within one year after surgery, according to the 2024 Heart Disease and Stroke Statistics: A Report of U.S. and Global Data From the American Heart Association. mg twice daily) combined with low-dose aspirin (81 mg daily).
BACKGROUND:Advanced chronic kidneydisease is associated with high cardiovascular risk, even after kidney transplant. Most were male (58%), median age was 58 years, and there was a high burden of hypertension (88%) and diabetes (33%). Circulation: Cardiovascular Imaging, Volume 17, Issue 1 , Page e015858, January 1, 2024.
Salvatore Carbone, PhD: First, I’d like to point out that obesity is a major risk factor for cardiometabolic disease. There are significant data that show that if you have obesity, you have a high risk of developing coronary heart disease, heart failure, type 2 diabetes (T2D) or risk factors such as hypertension and dyslipidemia. [1]
Overall, it appears that rhythm control strategy in AF may be better in those with heart failure and in those with associated cardiovascular conditions and early AF.
“Prior studies have shown cardiovascular disease in persons living with HIV, however not at such an early stage,” said senior author Ahmed M. senior clinical investigator, and director of the Biomedical and Metabolic Imaging Branch, National Institute of Diabetes and Digestive and KidneyDiseases ( NIDDK ), in Bethesda, Maryland.
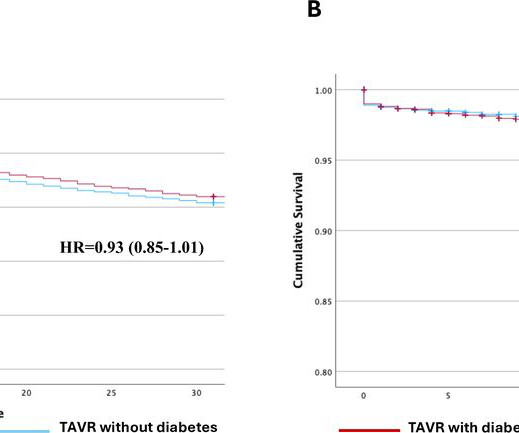
We aimed to examine the impact of diabetes on 30-day mortality, 30-day readmission and compare outcomes between TAVR and sAVR. Diabetes was present in 36.4% However, sAVR patients with diabetes had a higher adjusted risk of 30-day mortality (aHR=1.13 (1.01–1.25)) but not readmission (aHR=0.92 (0.84–1.01)).
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

















Let's personalize your content