This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
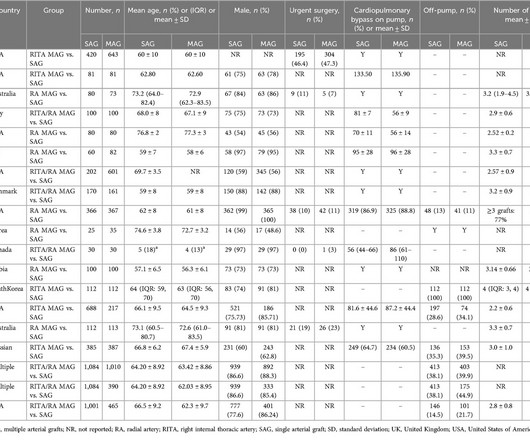
Observational studies and randomised controlled trials (RCTs) have yielded conflicting results regarding the outcomes of multiple arterialgrafts (MAG) vs. single arterialgrafts (SAG) in coronaryarterybypassgraft (CABG) surgery.
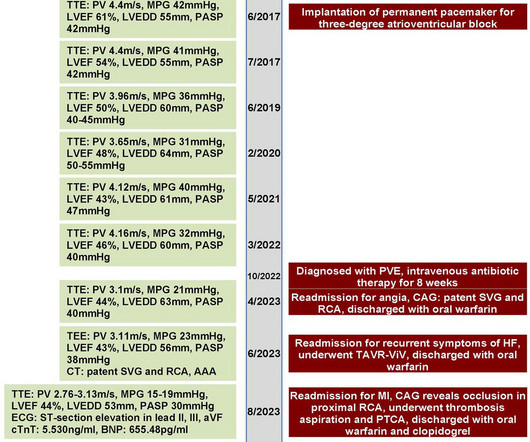
A 70-year-old female patient with a history of bioprosthetic aortic valve replacement and coronaryarterybypassgraft presented with bioprosthetic valve failure secondary to prosthetic valve endocarditis. This resulted in early death due to myocardialinfarction and acute heart failure.
Both indexes have been extensively validated in clinical trials in guiding revascularisation in patients with stable ischaemic heart disease undergoing percutaneous coronary intervention (PCI) with improved clinical outcomes. However, the role of these tools in coronaryarterybypassgrafting (CABG) is less clear.
Myocardialinfarction is among the top causes of mortality worldwide. Infarct-related torsade de pointes (TdP) is an uncommon complication. In the context of myocardialinfarction, coronaryarterybypassgraft (CABG) surgery is the prevalent therapeutic modality associated with several early and late complications.
BackgroundPrevious studies proposed the predictive value of baseline serum uric acid (SUA) in the prognosis of coronaryarterybypassgrafting (CABG) patients. The cutoff values of SUA increases in the overall population were 54.5 µmol/L µmol/L for in-hospital all-cause death and 42.6 µmol/L
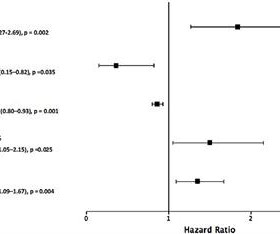
BACKGROUND:Diabetes may be associated with differential outcomes in patients undergoing left main coronary revascularization with percutaneous coronary intervention (PCI) or coronaryarterybypassgrafting (CABG). 1.52]) or without (155/1634 [9.7%] versus 142/1655 [8.9%]; hazard ratio, 1.08 [95% CI, 0.86–1.36;PintHR=0.87)
Objective To investigate the incidence and mortality risk associated with postdischarge major bleeding after coronaryarterybypassgrafting (CABG), and relate this to the incidence of, and mortality risk from, postdischarge myocardialinfarction. Median follow-up was 6.0 range 0–11) years. 95% CI 3.4
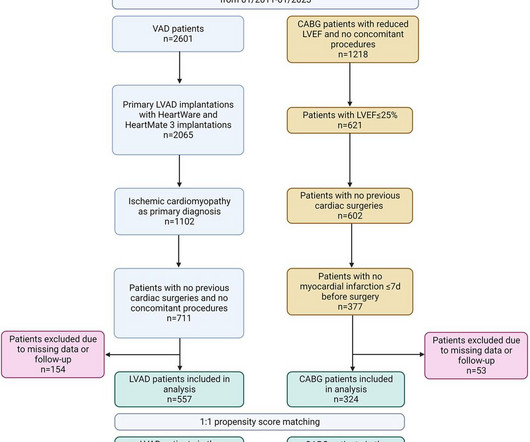
In this setting, implantation of a durable left ventricular assist device (LVAD) might be an alternative.MethodsWe retrospectively compared the outcomes of adult patients with CAD and a left ventricular ejection fraction (LVEF) ≤ 25% who underwent coronaryarterybypassgrafting (CABG) vs. LVAD implantation.
IPTW-adjusted Kaplan–Meier estimates by study group were calculated for all-cause mortality, stroke, the risk of repeat revascularization and myocardialinfarction up to a maximum follow-up of 10 years. Results MIDCAB patients had less rethoracotomies ( n = 13/3.6% vs. n = 30/8.0%, p = 0.012), fewer transfusions (0.93 units ± 1.83
In the ISCHEMIA (International Study of Comparative Health Effectiveness with Medical and Invasive Approaches) trial, researchers examined the risk of ischemic events in patients with stable coronaryartery disease. years, with 57.1% occurring within 30 days after CABG.
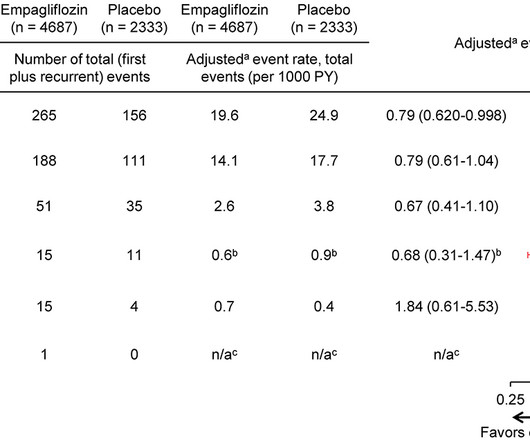
Background The effect of empagliflozin, a sodium-glucose-co-transporter-2 inhibitor, on risk for myocardialinfarction has not been fully characterized. MIs could be assigned to > 1 type.
Left main coronaryartery disease (CAD) and diabetes pose significant challenges in cardiovascular care, often leading to adverse outcomes. However, the comparative long-term efficacy of percutaneous coronary intervention (PCI) versus coronaryarterybypassgrafting (CABG) in patients with these conditions remains unclear.
The patient was transferred to the intensive care unit and received comprehensive treatment, including anticoagulation, myocardial nutritional support, improvement of cardiac function, continuous renal replacement therapy, organ function protection, anti-inflammatory treatment, and rehabilitation.
What are the long-term outcomes of percutaneous coronary intervention (PCI) versus coronaryarterybypassgrafting (CABG) in patients with non-ST-segment elevation myocardialinfarction (NSTEMI) and multivessel disease?
The overall prevalence of arterial hypertension was 33.2%, hyperlipidemia, 26.9%, smoking, 17.8%, and diabetes, 3.9%. of the patients were diagnosed with non-ST elevated myocardialinfarction (NSTEMI), 36.8% The left anterior descending artery (LAD) was the most common culprit lesion in 51% of the patients.
This study investigates the relationship between baseline 5-HTP levels and the incidence of major adverse cardiovascular events (MACE) in patients who have experienced ST-elevation myocardialinfarction (STEMI).Objective:Our years, 53 women) followed for up to 15 years.
Introduction The presence of non-coronary atherosclerosis (NCA) in patients with coronaryartery disease is associated with a poor prognosis. We have studied whether NCA is also a predictor of poorer outcomes in patients undergoing coronaryarterybypassgrafting (CABG).
Self-reported smoking status was assessed at each consecutive visit and used to determine smoking cessation after each interim ASCVD event (myocardialinfarction, percutaneous coronary intervention, coronaryarterybypassgraft, stroke/transient ischemic attack, peripheral artery disease).
Cox proportional hazard regression was used to evaluate the effect of Lp(a) on AVR, AVR or cardiac death, and valvular or cardiovascular events (AVR, cardiac death, myocardialinfarction, stroke, heart failure, or coronaryarterybypassgrafting). The maximal followup time was set to 5 years.
Nearly 65% of beneficiaries had a percutaneous coronary intervention, 33.5% had an acute myocardialinfarction, 17.5% had a coronaryarterybypassgraft, and 16.8% had a heart valve repair/replacement. Compared with nonparticipants, participants had 47.6
The primary outcome was risk of an ASCVD hospitalization composite outcome (myocardialinfarction, coronaryarterybypassgraft, percutaneous coronary intervention, stroke, transient ischemic accident) after COPD hospitalization relative to before COPD hospitalization.
The secondary outcomes comprise the odds of adverse events, including myocardialinfarction, ischemic stroke, transient ischemic attack (TIA), occlusive atherosclerotic disease, percutaneous coronary intervention, and coronaryarterybypassgraft (CABG)., The hemophilia cohort was slightly older (63.2[16.8]
This study is designed to evaluate the Corrie Hybrid CR, a technology‐based, multicomponent health equity‐focused intervention as an alternative to traditional in‐center CR among patients recovering from a cardiac event, surgery, or procedure compared with usual care alone.MethodsThe mTECH‐Rehab (Impact of a Mobile Technology Enabled Corrie CR Program) (..)
A rate of 15% of major depressive disorder has been reported in patients after myocardialinfarction or coronaryarterybypassgrafting, and this rate is >20% in patients with heart failure and is much higher in advanced heart failure.”
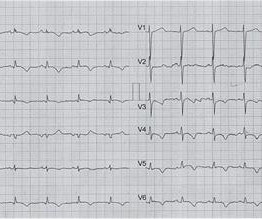
Angiography done after initial stabilization showed severe stenosis of distal left main coronaryartery. In addition, there were multiple lesions in all three vessels, making a standard indication for an urgent coronaryarterybypassgrafting. There is minimal ST segment elevation in aVR as well.
This is diagnostic of myocardialinfarction. Spontaneous CoronaryArtery Dissection Spontaneous coronaryartery dissection (SCAD) is an infrequent but increasingly recognized cause of acute coronary syndrome (1- 4%) 1 , most commonly affecting women (90%) 2. She felt more comfortable being admitted.
In most cases, rather, the culprit is gross ischemia due to myocardialinfarction, cardiomyopathy, or advanced coronaryartery disease. Unfortunately, today’s case is lacking any such diagnostics, thus I cannot say with certainty that the QT interval is, or is not, culpable in arrhythmogenesis. [1]
Author continued : STE in aVR is often due to left main coronaryartery obstruction (OR 4.72), and is associated with in-hospital cardiovascular mortality (OR 5.58). myocardialinfarction), arrhythmias, valvular pathology, shunts, or outflow obstructions.
Using the nationwide registries, we obtained information on admissions, prescriptions, educational length, and occupational status for both the AAS users and controls.
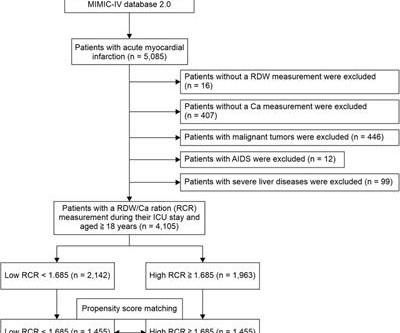
Objective Red cell distribution width (RDW) and serum calcium (Ca) levels are predictors of in-hospital mortality in acute myocardialinfarction (AMI) patients. However, their sensitivity and specificity are limited.
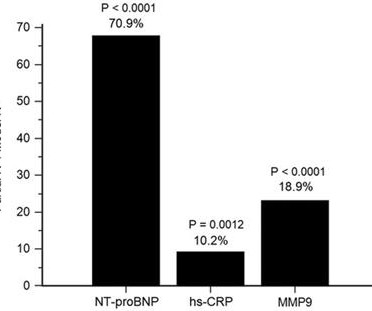
Introduction Matrix metalloproteinases (MMPs) and tissue inhibitors of metalloproteinases (TIMPs) have been linked to clinical outcomes in patients with coronaryartery disease (CAD). However, the prognostic value of TIMP-1 in patients with CAD who underwent coronaryarterybypassgrafting (CABG) has not been elucidated.
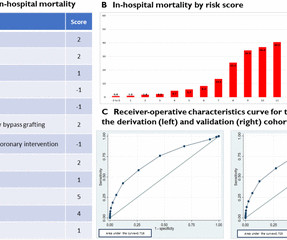
Background Takotsubo cardiomyopathy (TC) is an established differential diagnosis of myocardialinfarction with non-obstructive coronaries with significant interest but limited data on prognostication. We reviewed the characteristics and in-hospital outcomes and developed a novel risk score for TC. to 1.66), p<0.001).
years, 13 538 participants had incident CAD (myocardialinfarction, coronaryarterybypassgrafting, or coronary angioplasty).Results:TheLPAregion Plasma Lp(a) levels were measured and a CAD-PRS was calculated using the LDpred2 algorithm. Over the median follow-up of 12.6
One of the most effective treatments for severe coronaryartery disease, a type of cardiovascular disease, is coronaryarterybypassgrafting (CABG), a procedure designed to restore blood flow to the heart. But does coronaryarterybypass surgery also improve erectile capacity?
Adult Cardiac Surgery Database Lead Author Title Publication Date Jacob Raphael Red Blood Cell Transfusion and Pulmonary Complications: The Society of Thoracic Surgeons Adult Cardiac Surgery Database Analysis The Annals of Thoracic Surgery January 2024 Joseph Sabik Multi-Arterial versus Single-ArterialCoronary Surgery: Ten Year Follow-up of One Million (..)
Program Designations Access and Publications (A&P) 1 Participant User File (PUF) 2 Task Force on Funded Research (TFR) 3 Special Projects 4 Adult Cardiac Surgery Database Lead Author Title Publication Date William Keeling 2 National Trends in Emergency CoronaryArteryBypassGrafting European Journal of Cardiothoracic Surgery October 2023 Jake (..)
BACKGROUND:Sex differences in acute myocardialinfarction treatment and outcomes are well documented, but it is unclear whether differences are consistent across countries. for males; Israel percutaneous coronary intervention in 2018, 76.7% 1 in 2011 and 1.73:1 1 in 2018; Israel NSTEMI ratio, 1.71:1 1 in 2011 and 2.11:1
Coronaryarterybypassgrafting (CABG) is a common and effective treatment for patients with complex coronaryartery disease. This case report discusses a 75-year-old male patient who presented with angina and shortness of breath due to thrombus formation in a venous graft 20 years after CABG.
He had undergone coronaryarterybypassgrafting due to myocardialinfarction and severe three-vessel coronaryartery disease. Clinical introduction A man in his 80s presented to the hospital with dizziness, pre-syncope, chest tightness and palpitations for 3 days.
Primary endpoints included overall mortality, cardiac-related mortality, stroke, myocardialinfarction, repeat revascularization. Intraoperative transit time flow measurement (TTFM) was also analyzed.ResultsThe mean age of the cohort was 67.88.7 years, with 75.9% (85/112) being male.
This is the c ulprit for the patient's non-ST elevation myocardialinfarction AV groove circumflex, proximal LPDA, and mid LAD stenoses may also be hemodynamically significant Occlusion of the proximal nondominant RCA is not likely clinically relevant. Smith: not sure why that is. The ECG shows inferior ischemia.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






































Let's personalize your content