This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
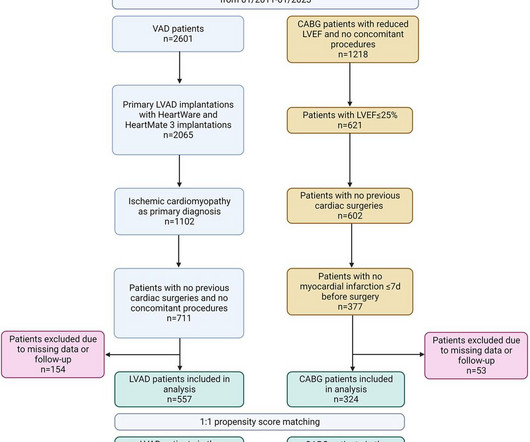
In this setting, implantation of a durable left ventricular assist device (LVAD) might be an alternative.MethodsWe retrospectively compared the outcomes of adult patients with CAD and a left ventricular ejection fraction (LVEF) ≤ 25% who underwent coronaryarterybypassgrafting (CABG) vs. LVAD implantation.
Increased Blood Clot Risk: Smoking enhances the bloods clotting tendency, raising the risk of heart attacks and strokes. These factors contribute to a host of cardiovascular problems, including coronaryartery disease, heartfailure, and arrhythmias, making smokers significantly more vulnerable to heart-related illnesses.
Background Heartfailure (HF) remains a major public health problem with a high mortality and morbidity worldwide. Currently, there is no optimal revascularisation strategy for patients with ischaemic cardiomyopathy despite suggestions that coronaryarterybypassgraft (CABG) may be superior to medical therapy in improving survival.
Patient underwent surgical closure of fistula and a 2-vessel coronaryarterybypassgraft surgery, with a LIMA pedicle graft to the LAD, and SV graft to the LCx.Postoperatively, patient was continued on medical therapy with improvement of symptoms. CCF can be congenital or acquired and has many variations.
Survival outcomes were equivalent between MAG and SAG for patients aged 80 years or older, and those with severe heartfailure , renal failure, peripheral vascular disease, or obesity.
Author continued : STE in aVR is often due to left main coronaryartery obstruction (OR 4.72), and is associated with in-hospital cardiovascular mortality (OR 5.58). In cardiogenic shock, fluid may worsen the pulmonary edema associated with acute heartfailure, but may still be required to support the hemodynamic status of the patient.
A 70-year-old female patient with a history of bioprosthetic aortic valve replacement and coronaryarterybypassgraft presented with bioprosthetic valve failure secondary to prosthetic valve endocarditis. This resulted in early death due to myocardial infarction and acute heartfailure.
In the ISCHEMIA (International Study of Comparative Health Effectiveness with Medical and Invasive Approaches) trial, researchers examined the risk of ischemic events in patients with stable coronaryartery disease. years, with 57.1% occurring within 30 days after CABG.
The outcomes of interest were all-cause death and major adverse cardiovascular events (MACE), including acute coronary syndrome (ACS), heartfailure (HF), need for additional revascularization, target vessel revascularization (TVR), SCAD recurrence, and stroke. There were initially 65.2%
to 7.09), p<0.001) and chronic heartfailure (OR 1.60 (95% CI 1.54 Factors significantly associated with TC were female sex (OR 6.78 (95% CI 6.47 to 1.66), p<0.001).
Cox proportional hazard regression was used to evaluate the effect of Lp(a) on AVR, AVR or cardiac death, and valvular or cardiovascular events (AVR, cardiac death, myocardial infarction, stroke, heartfailure, or coronaryarterybypassgrafting). The maximal followup time was set to 5 years.
A rate of 15% of major depressive disorder has been reported in patients after myocardial infarction or coronaryarterybypassgrafting, and this rate is >20% in patients with heartfailure and is much higher in advanced heartfailure.”
The proportion of coronaryarterybypassgraft and valvular intervention were comparable between patients with and without OSA. Compared to patients without OSA, patients with OSA were much older ( 44.00 ± 12.18 vs. 52.22 ± 10.33 vs. 26.32 ± 3.00 During a median follow-up of 23.1
We hypothesize the presence of comorbid cardiac disease has a synergistic effect on cognitive impairment in patients with asymptomatic CAS.Methods:Patients with 80% internal carotid artery stenosis with no history of stroke were recruited from inpatient and outpatient practices at a single, large, comprehensive stroke center.
Adult Cardiac Surgery Database Lead Author Title Publication Date Jacob Raphael Red Blood Cell Transfusion and Pulmonary Complications: The Society of Thoracic Surgeons Adult Cardiac Surgery Database Analysis The Annals of Thoracic Surgery January 2024 Joseph Sabik Multi-Arterial versus Single-ArterialCoronary Surgery: Ten Year Follow-up of One Million (..)
Program Designations Access and Publications (A&P) 1 Participant User File (PUF) 2 Task Force on Funded Research (TFR) 3 Special Projects 4 Adult Cardiac Surgery Database Lead Author Title Publication Date William Keeling 2 National Trends in Emergency CoronaryArteryBypassGrafting European Journal of Cardiothoracic Surgery October 2023 Jake (..)
Using the nationwide registries, we obtained information on admissions, prescriptions, educational length, and occupational status for both the AAS users and controls.
Introduction:Atrial fibrillation (AF) is a common cardiac arrhythmia, the risk of cardiovascular adverse outcome rises when it coexists with acute coronary syndrome (ACS) or undergoing percutaneous coronary intervention (PCI). The restrictive cubic spline in Figure 2 showed that LVEDD greater than 60 mm increased the risk of MACEs.
Anything that causes pulmonary edema: poor LV function, fluid overload, previous heartfailure (HFrEF or HFpEF), valvular disease. The patient was again sent home with a plan for surgical aortic valve replacement and coronaryarterybypassgrafting to the PDA. What other pathology is possible?
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






















Let's personalize your content