This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Finally, do a coronaryangiogram Possible alternative to pacing is to give a beta-1 agonist to increase heart rate. Even with tachycardia and a paced QRS duration of ~0.16 Use Lidocaine instead (lidocaine prevents the PVCs which cause R on T, and does not prolong the QT.) Dobutamine is an acceptable alternative. (J
A CT Coronaryangiogram was ordered. Here are the results: --Minimally obstructive coronary artery disease. --LAD Although a lesion is not visible anatomically on this CT scan, coronary catheter angiography could be considered based on Cardiology evaluation." A repeat troponin returned at 0.45 CAD-RADS category 1. --No
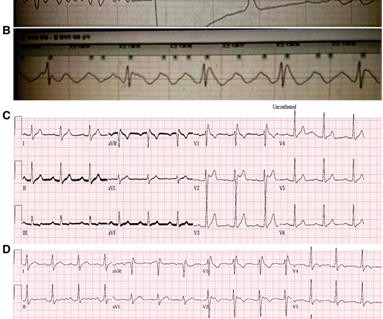
He was haemodynamically stable (BP 100/60) in the emergency room and had monomorphic ventricular tachycardia (VT) in the ECG. His coronaryangiogram (CAG) is shown in figure 1 ( ). His coronaryangiogram (CAG) is shown in figure 1 ( ). Figure 1 (A–C) Coronaryangiogram of left and right coronary arteries. (D)
Will you accept this patient for emergent coronaryangiogram based on the ECG changes? Putting all the findings together; dyspnea, slight tachycardia, delayed R-wave progression, prominent lateral S waves and ST depression maximal where the P waves are largest all point toward pulmonary disease as the cause of the ECG findings.
Given the rapid rate of the tachycardia and the amorphous shape of the QRS — the decision was made to sedate the patient and cardiovert. This phenomenon may sometimes be seen following an episode of a sustained tachycardia — in which marked ST-T wave abnormalities not due to infarction may be seen for a period of hours, or even days!
Category 1 : Sudden narrowing of a coronary artery due to ACS (plaque rupture with thrombosis and/or downstream showering of platelet-fibrin aggregates. It’s judicious, then, to arrange for coronaryangiogram. Supply-demand mismatch (non-occlusive coronary disease, or exacerbation of preexisting flow insufficiency) a.
Sent by Dan Singer MD, written by Meyers, edits by Smith A man in his late 30s presented with acute chest pain and normal vitals except tachycardia at about 115 bpm. As Ken says below, tachycardia is not common in OMI and distorts the ST segment, so managing the tachycardia and repeating the ECG is a good strategy.
From afar, there is gross tachycardia, cadence irregularities, and narrow QRS complexes that may, or may not, be Sinus in origin; and finally – a cacophony of wide complexes that might very well be ventricular in origin. McLaren : We’ve answered the first question – Sinus Tachycardia with episodic runs of wide QRS (RBBB morphology) and PVC’s.
The shortened PR-interval, specifically, proved to be quite beguiling as it swept crews down a differential diagnosis of intermittent accessory pathway syndrome – insomuch as a “syndrome” of recurrent tachycardia to account for the patient’s symptoms. Learning points 1] Acute Coronary Syndrome has many shades of clinical manifestation.
A coronaryangiogram was done that did not show significant coronary artery disease. But there are 3 other wide beats in the tachycardia that begins with beat #6 ( = beats #7; 13,14 ). Post ROSC the patient was alert and cooperative. Echocardiography showed apical ballooning with hypokinesis.
Ct coronaryangiogram showed normal coronary arteries. Smith note: I think CT coronaryangiogram is reasonable with the elevated troponins and symptoms. T-wave inversions and dynamic ST elevation Tachycardia, hyperthyroid, and ST elevation. He was diagnosed with mild AKI which resolved. What is it?
We investigated the incidence of an acutely occluded coronary in patients presenting with STE-aVR with multi-lead ST depression. All electrocardiograms (ECGs) and coronaryangiograms were blindly analyzed by experienced cardiologists. A slightly prolonged QTc ( although this is difficult to assess given the tachycardia ).
I find AV dissociation in VT to be very difficult to differentiate from artifact, as there are always random blips on tachycardia tracings. Cardiology was consulted and the patient underwent coronaryangiogram which showed diffuse severe three-vessel disease. Coronaryangiogram shows diffuse severe three-vessel disease.
The diagnostic coronaryangiogram identified only minimal coronary artery disease, but there was a severely calcified, ‘immobile’ aortic valve. Aortic angiogram did not reveal aortic dissection. 3) Anemia, or poisons of hemoglobin such as methemoglobin or CO 4) Fixed coronary stenosis that limits flow.
Patients with BrS can be asymptomatic or present with symptoms secondary to polymorphic ventricular tachycardia or ventricular fibrillation. The routine laboratory results, imaging study, coronaryangiogram, and echocardiogram (ECG) were normal. The patient did not have underlying diseases.
There is appreciable STE aVR with near-global STD that appropriately maximizes in Leads II and V5, and thus suggesting a circumstance of generic, diffusely populated, circumferential subendocardial ischemia versus occlusive coronary thrombus. [1] It’s judicious, then, to arrange for coronaryangiogram. Does the ECG normalize?
The status of the patients chest pain at this time is unknown : EKG 1, 1300: There is sinus tachycardia and artifact of low and high frequency. However, there is also significant tachycardia , with heart rate of 116, and known hypoxia. Acute coronary occlusion and acute pulmonary edema can coexist.
Angiogram Door to balloon time was 120 minutes (much too long) because of time taken for a CT. Coronaryangiogram showed 100% mid LAD occlusion for which she received a DES with excellent angiographic result. It was not SCAD (coronary dissection) Highest troponin I was 37,000 ng/L, but it was not measured to peak.
One big chunk of ACS-UA is secondary UA where there is increased demand as in stable angina with tachycardia*. we can witness menacingly deep resting ST depression with absolutely no thrombotic process going on in the coronary. Mind you, even a coronaryangiogram will not bail you out in terms of decision-making and risk prediction.
During observation in the ED the patient had multiple self-terminating runs of Non-Sustained monomorphic Ventricular Tachycardia (NSVT). CT coronaryangiogram showed a hypoplastic RCA and dominant LCx. This patient very likely has some form of idiopathic ventricular tachycardia. No PVCs are seen.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


























Let's personalize your content