This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Post cath ECG: Now there are hyperacute T-waves again, and recurrent ST depression in V2 This ECG would normally diagnostic of OMI until proven otherwise No further troponins were measured, but it looks like there is recurrent OMI Next day: A CT CoronaryAngiogram was done (CTCA) CARDIAC MORPHOLOGY AND FUNCTION: 1. IMPRESSION: 1.
A CT Coronaryangiogram was ordered. Here are the results: --Minimally obstructive coronary artery disease. --LAD LAD plaque with 0-25 percent stenosis. The LAD has moderate 40% ostial-proximal LAD stenosis and severe 90% mid LAD stenosis involving first diagonal branch. --The CAD-RADS category 1. --No
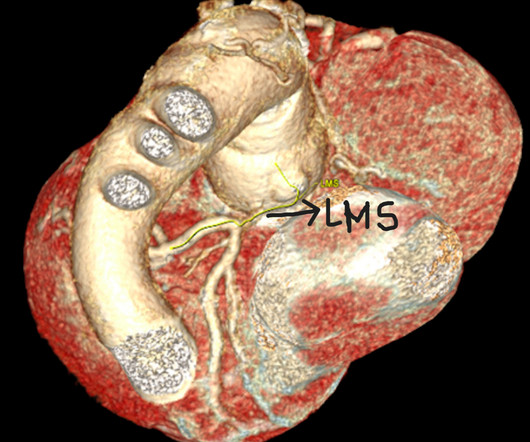
CT coronaryangiogram revealed severe narrowing of the left main coronary artery. Six months following modified Bentall procedure a patient presented with angina and acute ST depression. Minimal invasive off p.
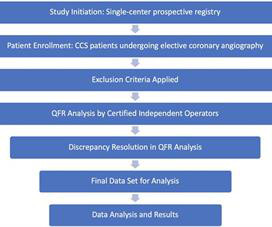
Methods This single-center prospective registry included consecutive patients with chronic coronary syndrome (CCS) who underwent elective coronary angiography, with or without revascularization. Average diameter stenosis (DS) was 37 ± 34%, and QFR was 0.87 ± 0.15, demonstrating a moderate correlation ( r = −0.84; 95% CI: −0.86
Or is it a very tight stenosis that does not allow enough flow to perfuse myocardium that has a high oxygen demand from severely elevated BP? The T waves in leads II and aVF have deflated, and the T wave in lead III has become terminally negative. The ST depressions in I and aVL have resolved.
Category 1 : Sudden narrowing of a coronary artery due to ACS (plaque rupture with thrombosis and/or downstream showering of platelet-fibrin aggregates. It’s judicious, then, to arrange for coronaryangiogram. Supply-demand mismatch (non-occlusive coronary disease, or exacerbation of preexisting flow insufficiency) a.
Case:A 74-year-old male with a recent NSTEMI presented for elective coronary artery revascularization. After placing temporary transvenous pacing and inserting sheaths in the right radial and right femoral arteries, both the RPL and RPD were wired with coronary guidewires.
Coronary angiography revealed a tortuous and extremely aneurysmal RCA, as well as multivessel coronary artery disease (mvCAD) involving LAD, D1, LCx, OM1. Notably, the LAD had multiple aneurysmal segments and areas of eccentric stenosis upto 90%.Multislice
The diagnostic coronaryangiogram identified only minimal coronary artery disease, but there was a severely calcified, ‘immobile’ aortic valve. Aortic angiogram did not reveal aortic dissection. Oxygen supply is determined by: 1) oxygen carrying capacity, 2) O2 saturation, and 3) Coronary flow.
She had a prior history of "NSTEMI" one month ago, during which she had a coronaryangiogram reportedly showing no stenosis in any coronary artery. Her vitals were within normal limits. Here is her triage ECG: PM Cardio Version (see original screenshot I received below) Original image.
History sounds concerning for ACS (could be critical stenosis, triple vessel), but differential also includes dissection, GI bleed, etc. 2 cases of Aortic Stenosis: Diffuse Subendocardial Ischemia on the ECG. We investigated the incidence of an acutely occluded coronary in patients presenting with STE-aVR with multi-lead ST depression.
There is ventricular hypertrophy in the absence of abnormal loading conditions, such as aortic stenosis, or hypertension, for example – of which the most common variant is Asymmetric Septal Hypertrophy. Type II MI), however decided to pursue coronaryangiogram out of an abundance of caution.
The coronaryangiogram revealed no critical stenosis, or acute plaque ulceration. Takotsubo should be a diagnosis of exclusion after angiography reveals no obstructive coronary disease, and repeat Echo displays left ventricular recovery. Furthermore, pertinent electrolyte values (e.g.
During angiogram in the cath lab, the patient suffered two episodes of ventricular fibrillation for which he was successfully defibrillated. Angiogram showed a culprit lesion of 100% stenosis to the right coronary artery and 100% stenosis of the right posterior descending artery, both with TIMI 0 flow.
Advanced multi-vessel disease was found with stents deployed to the mid-LCx (80% stenosis), D1 (90% stensosis), and the pLAD (95% stenosis). It’s judicious, then, to arrange for coronaryangiogram. elevated BP), but rather directly correlated with coronary obstruction and stymied TIMI flow. Does the ECG normalize?
On the other hand, the murmur in valvular aortic stenosis does not change substantially or decreases slightly following the Valsalva maneuver. A decrease in intensity, due to attenuation of obstruction, is heard after going from a standing to a sitting or squatting position, with a handgrip, and following passive elevation of the legs.
Diamond and Forrester accomplished this by first establishing the prevalence of coronary artery disease based on how clinically likely patients with chest pain symptoms were found to have coronary disease based on a coronaryangiogram. The results of this dataset by age and gender follow.
More troponin values were measured at the cardiac center: 2327- 267 ng/L 0821- 355 ng/L 1108- 305 ng/L An echocardiogram on day three of the patients admission showed an ejection fraction of 46% with abnormal basal inferior and basal lateral segments, and severe aortic stenosis. What "initiates" the aortic stenosis cascade?
In this case, it is possible that the physicians interpreted the ST depression in anterior leads as subendocardial ischemia of the anterior wall, and the mid LAD stenosis as the culprit of that ischemia. Subendocardial ischemia does not localize. This was likely a case of wrong-vessel PCI. This is surprisingly common.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
























Let's personalize your content