This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
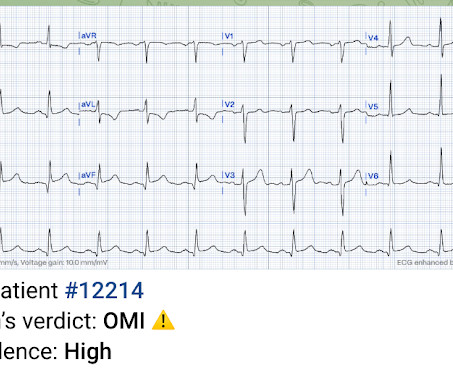
Post cath ECG: Now there are hyperacute T-waves again, and recurrent ST depression in V2 This ECG would normally diagnostic of OMI until proven otherwise No further troponins were measured, but it looks like there is recurrent OMI Next day: A CT CoronaryAngiogram was done (CTCA) CARDIAC MORPHOLOGY AND FUNCTION: 1. IMPRESSION: 1.
Wuhan Asia Heart Hospital, Wuhan, China Did you guess the diagnosis correctly? It is an acceptable diagnosis, if you thought an anomalous LCA, a LAD CTO or a single coronary artery. Video source and courtesy: Leizhi Ku,, Xiaojing Ma, From the Departments of Radiology (L.K.) and Echocardiography (X.M.), It is left main atresia.
So the patient was admitted to the hospital with no plan for an angiogram. The Queen of Hearts now sees no OMI with low confidence: The patient did not receive an angiogram on day two of his hospitalization because the cath lab was too busy. Instead he had an angiogram at 0800 on day 3. Smith: What???!!!
A Coronaryangiogram from 8 years prior revealed that he had had an inferior posterior STEMI at the time due to 100% occlusion of the proximal RCA. The above said — I thought it may be insightful to review the initial pre-hospital ECG , which has to be interpreted as an acute OMI until proven otherwise.
This was texted to me from a former resident, while working at a small rural hospital, with the statement: "I can’t convince myself of anything here, but he’s a 63-year-old guy with prior stents and a good story for ACS." We don't know if he had a stress test, a CT Coronaryangiogram, or they just decided to do an angiogram.
It’s judicious, then, to arrange for coronaryangiogram. Coronary occlusion, however, might be present concurrently with subendocardial ischemia on the time-zero ECG, or evolve into such. Proximal LAD disease with/without a) and b) It seemed quite apparent that this was an Acute Coronary Syndrome. CoronaryAngiogram 1.
Hospital evaluation for this patient was negative for an acute coronary syndrome ( ie, CT coronaryangiogram was normal — troponin was not elevated — and Echo was negative, with no sign of pericardial effusion ). CT CoronaryAngiogram showed no sign of underlying coronary disease.
Could there have been a different outcome if the crews immediately recognized OMI – versus a shortened PR-interval – and commenced with pre-hospital Cath Lab activation? Learning points 1] Acute Coronary Syndrome has many shades of clinical manifestation. I don’t have an answer to this specific question.
Ct coronaryangiogram showed normal coronary arteries. Smith note: I think CT coronaryangiogram is reasonable with the elevated troponins and symptoms. He was given aspirin and heparin and transferred to the local cardiac center for further evaluation. He was diagnosed with mild AKI which resolved.
He was not interested in remaining hospitalized for further cardiac monitoring or inpatient EP consultation as he felt well, was convinced dehydration was the reason for his syncope, and he adamantly wanted to go home. Discussion Thus, no further ECGs were recorded and there was no angiogram or stress test or CT coronaryangiogram.
This worried the crew of potential acute coronary syndrome and STEMI was activated pre-hospital. When OMI is captured in this early phase, there exists the highest amount of salvageable myocardium and least likelihood of heart failure at hospital discharge. Smith comment : V5 and V6 are excessively discordant!!!!
We investigated the incidence of an acutely occluded coronary in patients presenting with STE-aVR with multi-lead ST depression. All electrocardiograms (ECGs) and coronaryangiograms were blindly analyzed by experienced cardiologists. Thirty-two patients (40%) had mild to moderate or no significant disease.
The diagnostic coronaryangiogram identified only minimal coronary artery disease, but there was a severely calcified, ‘immobile’ aortic valve. Aortic angiogram did not reveal aortic dissection. The patient was brought directly to the cardiac catheterization lab for PCI, bypassing the ED.
This final ECG, however, was recorded upon hospital arrival, the timing of which coincided with the patient verbalizing cessation of symptoms. Cardiology admitted him for observation with plans for next-day coronaryangiogram. The peak Troponin I confirmed myocardial infarction. (A 1] Driver, B.
Diamond and Forrester accomplished this by first establishing the prevalence of coronary artery disease based on how clinically likely patients with chest pain symptoms were found to have coronary disease based on a coronaryangiogram. and 1.7% [ P =0.43]; 12‐month: 0.6% Which is exactly what the numbers show.
He was then transferred to quaternary care childrens hospital. Repeat CT angio chest (not CT coronary, unclear what protocol) showed possible LAD aneurysm and thrombus. No apical thrombus noted using Definity contrast. Coxsackie serologies negative. Covid PCR negative. UDS positive for marijuana only.
Cardiology services were consulted at a PCI capable hospital. Case Continued The patient was discharged from the hospital with a plan for a scheduled coronaryangiogram to assess the coronary arteries and the possibility of aortic valve replacement. She was started on lasix.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





















Let's personalize your content