This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Background:Epicardial patch defibrillators (EPDs) were commonly implanted in the 1990s for secondary prevention of sudden cardiac death. A repeat CT angiogram indicated contrast extension into the ventricular myocardium near the EPD but no lung spillage suggestive of pseudoaneurysm (Picture 1B).She
Finally, do a coronaryangiogram Possible alternative to pacing is to give a beta-1 agonist to increase heart rate. Because she has cardiomyopathy and ventricular dysrhythmias, the pacer included an Implanted Cardioverter-Defibrillator (ICD) Echo 6 days later after CRT: Normal estimated left ventricular ejection fraction.
Workup including routine laboratory results, 12-lead electrocardiogram (ECG), echocardiogram, and coronaryangiogram was non-specific. During the intravenous lacosamide infusion, the patient developed sudden cardiac arrest caused by ventricular arrhythmias necessitating resuscitation. 2893C>T, p.Arg965Cys) in the SCN5A gene.
The routine laboratory results, imaging study, coronaryangiogram, and echocardiogram (ECG) were normal. For secondary prevention, the patient underwent implantable cardioverter defibrillator implantation. The patient did not have underlying diseases. A type 1 BrS pattern was identified in one resting ECG.
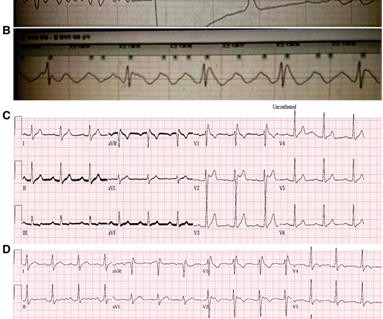
After resuscitation and defibrillation , there were no more episodes of TdP. A coronaryangiogram was done that did not show significant coronary artery disease. Below is the patient’s 12 lead ECG following defibrillation. Post ROSC the patient was alert and cooperative. What does this ECG tell you?
Despite immediate chest compressions, and multiple rounds of defibrillation, he could not be resuscitated. Learning points 1] Acute Coronary Syndrome has many shades of clinical manifestation. He became unconscious as the monitor displayed VF.
During angiogram in the cath lab, the patient suffered two episodes of ventricular fibrillation for which he was successfully defibrillated. Angiogram showed a culprit lesion of 100% stenosis to the right coronary artery and 100% stenosis of the right posterior descending artery, both with TIMI 0 flow.
We can, therefore, put down the defibrillation pads, set aside the amiodarone, and look further at the ECG. The coronaryangiogram revealed no critical stenosis, or acute plaque ulceration. Paradoxically, though, the third green arrow identifies a QRS that is more narrow than the RBBB complexes surrounding it.
CT coronaryangiogram showed a hypoplastic RCA and dominant LCx. Most patients can be managed without and implantable cardioverter defibrillator (ICD) In patients with PVCs/VT and a presentation not typical for an idiopathic origin cardiac magnetic resonance (CMR) should be considered, even if the Echo is normal.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.















Let's personalize your content