This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
In adults with congenital heart disease (ACHD patients), atrial arrhythmias (AA) and heart failure (HF) are common. 1 Factors related to congenital heart disease, such as underlying anatomy, surgical repair technique and scars, can all be considered as AA substrates.
The prevalence of congenital heart disease (CHD) in adult patients has risen with advances in diagnostic and surgical techniques. Macroreentrant atrial tachycardias, particularly cavotricuspid isthmus-dependent flutter, are frequently reported.
Ventricular tachycardia is a potentially life threatening cardiac arrhythmia. On the ECG, ventricular tachycardia can be defined as three or more ventricular ectopic beats occurring in a sequence at a rate more than 100 per minute. Another rare form of ventricular tachycardia is bidirectional ventricular tachycardia.
It should be kept in mind that on occasions, beta-one agonist can result in increased ventricular ectopy e.g., in severe myocardial ischemia (by increasing myocardial demand), or sometimes with congenital long-QT syndrome. Even with tachycardia and a paced QRS duration of ~0.16 J Am Coll Cardiol.
It has been used to treat both inappropriate sinus tachycardia and sinus tachycardia related to heart failure in children and adults. Ivabradine’s high selectivity and minimal side effects make it an attractive candidate for wider applications such as focal atrial tachycardia (FAT).
ECG Blog #422 and Blog #425 Cases with Congenital Heart Disease in Adults. ECG Blog #210 Reviews the Every-Other-Beat ( or Every-Third-Beat ) Method for estimation of fast heart rates and discusses another case of a regular WCT rhythm. ECG Blog #220 Review of the approach to the regular WCT ( = W ide- C omplex T achycardia ).
Three or more ventricular beats in a row at a rate above 100 per minute is termed ventricular tachycardia. Ventricular tachycardia lasting more 30 seconds or requiring termination earlier due to hemodynamic compromise is called sustained ventricular tachycardia. Either case, the treatment is ablation of the right bundle.
Atrial arrhythmias are an important source of morbidity in adults with congenital heart disease (CHD) and have been linked to sudden death in certain subgroups. Whereas intra-atrial reentrant tachycardia (IART) is the most common arrhythmia, the prevalence of atrial fibrillation (AF) is increasing.
A cardiac diverticulum is a rare congenital outpouching of the myocardial wall. We report a case of frequent non-sustained ventricular tachycardia (NSVT) originating from a diverticulum located in the right ventricular outflow tract (RVOT).
Blood Pressure Many medications used to treat congenital heart disease can affect blood pressure levels. A rapid heartbeat (tachycardia) can increase the workload on your heart, while a slow heartbeat (bradycardia) can cause fatigue and dizziness. Here are some key things for you and your healthcare team should keep an eye on: 1.
Tetralogy of Fallot (TOF) represents the poster child for monomorphic ventricular tachycardia (MVT) in congenital heart disease. Sustained MVT affects approximately 10% of such patients at 30 years after cardiac repair and is inextricably related to the burden of sudden cardiac death (SCD).(1)
Congenital heart disease is a daunting diagnosis for any parent. We’ll cover common types of medications used to treat congenital heart disease, what parents should know about their use, and potential side effects to watch out for. Be sure to talk to your doctor if you have any questions or concerns.
ABSTRACT Introduction Left atrial appendage aneurysm (LAAA) is a rare congenital cardiac anomaly that involves the progressive dilatation of the left atrial appendage (LAA), predisposing the patient to serious complications such as atrial tachyarrhythmias, life-threatening systemic thromboembolism, and cardiac dysfunction.
Abstract Introduction We report the case of an 18-year-old female with recurrent syncope that was discovered to have congenital long QT syndrome (LQTS) and episodes of a transiently short QT interval after spontaneous termination of polymorphic ventricular tachycardia.
All these features together in a cyanotic congenital heart disease is characteristic of tricuspid atresia. Ebstein’s anomaly may be associated with right sided accessory pathway in ventricular pre-excitation, that is WPW syndrome, with or without atrioventricular re-entrant tachycardia.
Evaluation of escape rates and ventricular ectopy with exercise in complete heart block is an important aspect in the evaluation of congenital complete heart block. ECG showing congenital complete heart block with ventricular rate of 47/min and atrial rate of 63/min. Tracing shows bidirectional ventricular ectopics.
An Initial ECG was performed: Initial ECG: Sinus tachycardia with prolonged QT interval (QTc of 534 ms by Bazett). She was admitted to the ICU where subsequent ECGs were performed: ECG at 12 hours QTc prolongation, resolution of T wave alternans ECG at 24 hours Sinus tachycardia with normalized QTc interval. No ischemic ST changes.
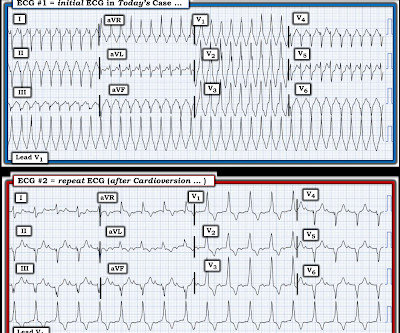
Because of this, it is uncommon to see sinus tachycardia with a prolonged PR interval. And I wish I had record of ECG monitoring just before — and during — and just after the rhythm changes from the regular tachycardia in ECG #1 — to the bigeminal rhythm in ECG #2. This is precisely what we see in Figure-6.
Abstract Introduction The use of flecainide and propafenone for medical cardioversion of atrial fibrillation (AF) and atrial flutter/intra-atrial reentrant tachycardia (IART) is well-described in adults without congenital heart disease (CHD).
Her clinical tachycardia was easily inducible and had a cycle length (TCL) of 340 ms. A 37-year-old woman with biventricular repair for pulmonary atresia and an intact ventricular septum was referred for an electrophysiological study in the context of recurrent atrial arrhythmias with multiple electrical cardioversions.
Catheter ablation is an established treatment for accessory pathway (AP)-related tachycardia 1. Multiple APs, congenital abnormalities and difficulties in catheter manipulation are particularly challenging situations. However, failed AP ablation is often due to a combination of inaccurate mapping and anatomically challenging APs.
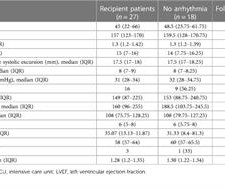
Introduction Heart transplantation (HT) is the only treatment option in children with heart failure secondary to cardiomyopathies and non-reparable congenital heart diseases. Two patients developed chronic sinus tachycardia at 4 and 16 months and were treated with Beta-blockers after eliminating all causes of sinus tachycardia.
Abstract Introduction Acquired Wolff–Parkinson–White (WPW) syndrome can occur after congenital heart disease (CHD) surgery. The first electrophysiology study (EPS) induced orthodromic atrioventricular reentrant tachycardia and successfully eliminated the posteroseptal accessory pathway (AP).
That said — physical exam findings of cyanosis and clubbing, together with the history of longstanding dyspnea episodes suggested more of a chronic problem ( presmably the expression of Congenital Heart Disease in an adult ) — rather than an isolated episode of VT in a young man.
There is a run of polymorphic ventricular tachycardia — which given the QT prolongation, qualifies as Torsades de Points ( TdP ). This patient was having recurrent episodes of polymorphic ventricular tachycardia with an underlying long QT interval ( = Torsades des Pointes ). ECG #2 Interpretation of ECG #2: Underlying sinus rhythm.
If this is in a child, or a young adult, you will think that this is juvenile T inversion and the heart block is congenital complete heart block, in which heart rate is usually better as it is supra Hisian and narrow QRS as junction will be controlling. Instead usually you will have ventricular tachycardia with AV dissociation.
Transcript of the video: Ebstein’s Anomaly is one of the cyanotic congenital heart disease in which survival to adult life is common. This is one important cause of supraventricular tachycardia in Ebstein’s anomaly. Electrophysiological study will show that, and this pathway can be ablated.
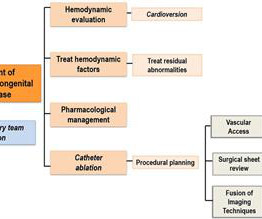
Methods Adult congenital heart disease (ACHD) clinicians (≥10 years of experience) participated (one cardiac surgeon and four cardiologists (two paediatric and two adult cardiology trained) with expertise in heart failure (HF), electrophysiology, imaging and intervention).
Initial vital signs include: NIBP 99/58 HR 150-160 (trend) RR 10 (spontaneous, but shallow) SpO2 86 (RA) BBS CTA The initial rhythm strip is attached: Figure 1 There is a wide complex tachycardia of varying morphology, amplitude, and R-R cycle length. genes implicated in congenital Long QT syndrome, such as SCN5A and KCNQ1). [1-3,
So a prominent A wave in a complex congenital heart disease situation would indicate that interventricular septum is intact. One is ventricular tachycardia with regular retrograde activation. Especially, in patients with rheumatic fever, PR interval is prolonged and there is sinus tachycardia. Second is junctional tachycarida.
A fast heartbeat is called tachycardia, while a slow heartbeat is called bradycardia in medical terms. Hypoplastic left heart syndrome is a common congenital heart defect in which there is a problem with the heart's blood supply, and the left side of the heart does not develop correctly.
The ECG shows sinus tachycardia, a narrow, low voltage QRS with alternating amplitudes, no peaked T waves, no QT prolongation, and some minimal ST elevation in II, III, and aVF (without significant reciprocal STD or T wave inversion in aVL). It is difficult to tell if there is collapse during diastole due to the patient’s tachycardia.
Answer : you must treat the patient's underlying condition causing sinus tachycardia, and repeat the ECG at the lower heart rate. Optimal QT interval correction formula in sinus tachycardia for identifying cardiovacular and mortality risk: Findings from the Penn Atrial Fibrillation Free study. which is 0.6 So is it really prolonged?
Background:Patients with adult congenital heart disease (ACHD) form a unique subset of patients with complex ventricular tachycardia (VT).Objective:To The primary composite outcome was recurrent monomorphic VT, and repeat ablation.Results:Out of 508 procedures for ventricular tachycardia ablation, 37 were performed in ACHD patients.
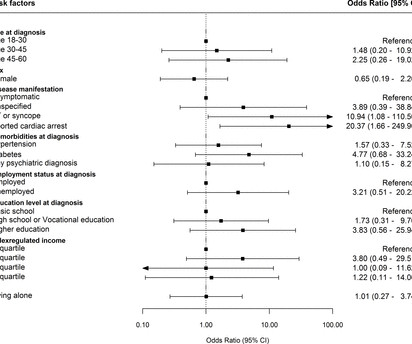
Objective To examine workforce attachment among patients with congenital long QT syndrome (cLQTS) following diagnosis and identify factors associated with workforce attachment. to 249.9); ventricular tachycardia/syncope OR 10.9 (95% 95% CI, 1.7 95% CI, 1.1 to 110.5)). No other associated factors were identified.
Atrioventricular nodal reentrant tachycardia (AVNRT) is a common supraventricular tachycardia in children and congenital heart disease (CHD) patients. Nowadays, in large enough children, chronic treatment for symptomatic and recurrent AVNRT episodes relies on transcatheter ablation.
It would probably tell us whether the abnormal QRS morphology that we see in Figure-1 is the result of VT vs SVT ( ie, with the abnormal QRS morphology being the result of the patients underlying Congenital Heart Disease ). That said, the PR interval generally shortens with tachycardia. As a technical point — the PR interval of 0.20
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




































Let's personalize your content