This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Ventricular tachycardia is a potentially life threatening cardiac arrhythmia. On the ECG, ventricular tachycardia can be defined as three or more ventricular ectopic beats occurring in a sequence at a rate more than 100 per minute. Another rare form of ventricular tachycardia is bidirectional ventricular tachycardia.
Three or more ventricular beats in a row at a rate above 100 per minute is termed ventricular tachycardia. Ventricular tachycardia lasting more 30 seconds or requiring termination earlier due to hemodynamic compromise is called sustained ventricular tachycardia. Either case, the treatment is ablation of the right bundle.
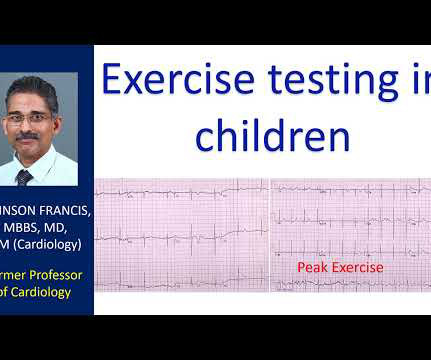
Evaluation of escape rates and ventricular ectopy with exercise in complete heart block is an important aspect in the evaluation of congenital complete heart block. ECG showing congenital complete heart block with ventricular rate of 47/min and atrial rate of 63/min. Tracing shows bidirectional ventricular ectopics.
If this is in a child, or a young adult, you will think that this is juvenile T inversion and the heart block is congenital complete heart block, in which heart rate is usually better as it is supra Hisian and narrow QRS as junction will be controlling. Instead usually you will have ventricular tachycardia with AV dissociation.
Transcript of the video: Ebstein’s Anomaly is one of the cyanotic congenital heart disease in which survival to adult life is common. This is one important cause of supraventricular tachycardia in Ebstein’s anomaly. Electrophysiological study will show that, and this pathway can be ablated.
So a prominent A wave in a complex congenital heart disease situation would indicate that interventricular septum is intact. One is ventricular tachycardia with regular retrograde activation. Especially, in patients with rheumatic fever, PR interval is prolonged and there is sinus tachycardia. Second is junctional tachycarida.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











Let's personalize your content