This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
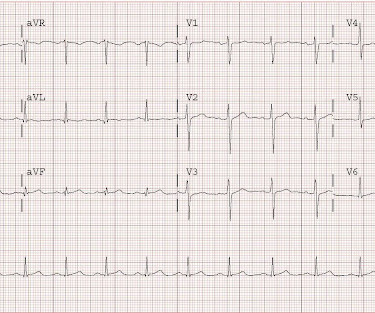
Written by Jesse McLaren A 70 year old with prior MIs and stents to LAD and RCA presented to the emergency department with 2 weeks of increasing exertional chest pain radiating to the left arm, associated with nausea. I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion.
This is all suggestive of posterior STEMI, but not definitely diagnostic. mm in only one posterior lead is highly sensitive and specific for posterior STEMI). Two stents were placed. ST depression in V1-V4, isolated, may be either posterior STEMI or NSTEMI. The ECG normalized overnight. Maximum troponin was 2.1
Echo on the day after admission showed EF of 30-35% and antero-apical wall akinesis with an LV thrombus [these frequently form in complete or near complete (no early reperfusion) anterior STEMI because of akinesis/stasis] 2 more days later, this was recorded: ST elevation is still present. An open 90% LAD was stented.
Subtle as a STEMI." (i.e., Given that this is before it is released into the circulation by reperfusion therapy, this is a massively elevated troponin. She was taken to the cath lab, where she was found to have 100% in-stent restenosis of the proximal LAD. None of the 20 ever evolved to STEMI criteria.
reports MI in 2001 with a stent placed in the "marginal" artery. First, this patient had a known stent in the "marginal" artery and thought he was having a heart attack. By definition, this is a non-STEMI because there is not 1 mm of ST elevation in 2 consecutive leads. Pain is similar, but associated with less SOB.
Precordial ST depression may be subendocardial ischemia or posterior STEMI. If you thought it might be a posterior STEMI, then you might have ordered a posterior ECG [change leads V4-V6 around to the back (V7-V9)]. So there was 3-vessel disease, but with an acute posterior STEMI. Circulation 2007;115(10):1306-24.
Step 1 to missing posterior MI is relying on the STEMI criteria. A prospective validation of STEMI criteria based on the first ED ECG found it was only 21% sensitive for Occlusion MI, and disproportionately missed inferoposterior OMI.[1] But it is still STEMI negative. A 15 lead ECG was done (below). In a study last year, 14.4%
But because there was no new ST elevation, the ECG was signed off as “STEMI negative” and the patient waited to be seen. But the ECG still doesn’t meet STEMI criteria. It was therefore interpreted as “no STEMI” and the patient was treated with dual anti-platelets and referred to cardiology as “NSTEMI.” the cardiologist 5.
Circulation, Volume 150, Issue Suppl_1 , Page A4125093-A4125093, November 12, 2024. Types of ACS include stable angina 5.3% (n=8), unstable angina 24% (n=36), NSTEMI 28.7% (n=43), and STEMI 24% (n=36). All patients had interventional PCI with balloon and stent insertion. The mean age of patients was 57.68 (SD= 11.19) years.
The "criteria" for posterior STEMI are 0.5 Is it STEMI or NonSTEMI? It was opened and stented with a door to balloon time of about 120 minutes (this is long for STEMI, but very short for a high risk Non STEMI). The 4th, after the opening of the artery and release of troponin from the cardiac circulation, was 99.9
The patient was brought to the ED as a possible Code STEMI and was seen directly by cardiology. Similarly, STEMI guidelines call for urgent angiography for refractory ischemia or electrical/hemodynamic instability, regardless of ECG findings. So the RCA was stented. Vitals were HR 58 BP 167/70 R20 sat 96%.
You've read in my previous posts that I have a lot of evidence that Wellens' represents spontaneously reperfused STEMI in which the STEMI went unrecorded. New ST elevation diagnostic of STEMI [equation value = 25.3 Circulation 1991;84:1454-1455. It was stented. Computerized QTc = 417.
Here is the prehospital ECG, with pain: Hyperacute anterolateral STEMI The medics had activated the cath lab and the patient went for angiogram and had a 95% stenotic LAD with TIMI-3 flow. A stent was placed. When the patient had chest pain, prior to nitroglycerine, what do you think the ECG showed ?
It is equivalent to a transient STEMI. Not much, but studies of STEMI and NonSTEMI show that about 70% of those diagnosed with STEMI have a peak troponin I above 10 ng/mL and that about 70% of those diagnosed with NonSTEMI have a peak troponin I below 10 ng/mL. The lesion was stented. Circulation. 2012;126:579–588.
The 50-something patient with history of coronary stenting and slightly reduced LV ejection fraction. In the setting of prior stenting and reduced left ventricular ejection fraction, would pursue a heart team revascularization approach Syntax score 28.5, This alone could be due to LVH, but V4 could NOT be due to LVH.
Compare to the anatomy after stenting: The lower of the 2 now easily seen branches is the circumflex, now with excellent flow. Circulation 2002; 105(4): 539-42. Here is his angiogram: This shot shows that the left circumflex (LCx) is occluded at the ostium (origin). This is seen just millimeters beyond the tip of the catheter.
Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? This was stented. Comments: STEMI with hypokalemia, especially with a long QT, puts the patient at very high risk of Torsades or Ventricular fibrillation (see many references, with abstracts, below).
Recall from this post referencing this study that "reciprocal STD in aVL is highly sensitive for inferior OMI (far better than STEMI criteria) and excludes pericarditis, but is not specific for OMI." Here is the angiogram after stent placement. Circulation , 130 (25). The case continues. A third EKG was performed around 8 AM.
This doesn’t meet STEMI criteria so in the current paradigm there’s no urgency to getting an angiogram. The initial ECG suggested either subacute or reperfused inferoposterior occlusion and clearly does not meet traditional STEMI criteria. Discharge diagnosis was ‘STEMI’, even though no ECG ever met STEMI criteria.
Circulation, Volume 150, Issue Suppl_1 , Page A4132742-A4132742, November 12, 2024. A random-effects model was used for outcomes with high heterogeneity.Results:We included 4 RCTs with 3173 patients comparing FFR-guided CR with culprit-only PCI in patients with STEMI and multivessel coronary artery diseases.
Circulation, Ahead of Print. The primary efficacy objective was to demonstrate superiority of PPA to reduce the primary efficacy end point of all-cause death, nonfatal myocardial infarction, nonfatal stroke, stent thrombosis (definite), or urgent revascularization (any vessel) within 30 days.
A middle-aged male with h/o CAD and stents presented with typical chest pressure. It may be difficult to read STEMI in the setting of RBBB. There is, however, a long QT also, with abnormal T-waves, but this is not STEMI. So there is pathologic ST elevation here, consistent with anterolateral STEMI. Called 911.
A male in late middle age with a history of RCA stent 8 years prior complained of chest pain. Here are three more dramatic cases that illustrate RBBB + LAFB Case 1 of cardiac arrest with unrecognized STEMI, died. EMS recorded the following ECG: What do you see?
When total LM occlusion does present with STE in aVR, there is ALWAYS ST Elevation elsewhere which makes STEMI obvious; in other words, STE is never limited to only aVR but instead it is part of a massive and usually obvious STEMI. All are, however, clearly massive STEMI. This is her ECG: An obvious STEMI, but which artery?
It was treated with and dual "kissing balloons" and drug eluting stents. Here is the post stent ECG: There is greater than 50% resolution of ST elevation (all but diagnostic of successful reperfusion) and Terminal T-wave inversion (also highly suggestive of successful reperfusion). Circulation 1993; 88:896-904. TIMI flow is 0.
After stent deployment, we often see improvement in the ST-T within seconds or minutes. Here is the final angiogram following placement of a stent in the ostial RCA. 2:04 PM, post stent deployment You can see that even after complete restoration of flow, the ECG still looks terrible, V most of all. Circulation , 92 (3), 657671.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
































Let's personalize your content