This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
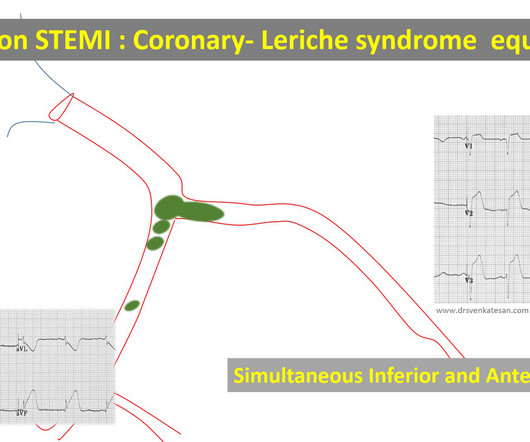
RCA-dependent LAD circulation through collaterals 3. True bifurcation STEMI with static thrombus (Carinal trapping of thrombus ,Coronary Lerish sydrome ) 4. Embolic STEMI with showers of emboli into both LCX and LAD Simultaneous or sequential Anterior and Inferior STEMI 5. Wrap around LAD true Global MI 2.
I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion. Non-STEMI guidelines call for “urgent/immediate invasive strategy is indicated in patients with NSTE-ACS who have refractory angina or hemodynamic or electrical instability,” regardless of ECG findings.[1]
Thus, this is both an anterior and inferior STEMI. How old is this antero-inferior STEMI? Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. Armstrong et al.)], the presence of such well developed anterior Q-wave suggests completed transmural STEMI. Circulation 1993;88(3):896-904.
Circulation, Volume 150, Issue Suppl_1 , Page A4142231-A4142231, November 12, 2024. Background:Little is known about the clinical relevance of interleukin (IL)-6 and the severity of patients with acute ST-elevation myocardial infarction (STEMI). All information about clinical and paraclinical parameters was recorded.
This is all suggestive of posterior STEMI, but not definitely diagnostic. mm in only one posterior lead is highly sensitive and specific for posterior STEMI). ST depression in V1-V4, isolated, may be either posterior STEMI or NSTEMI. A posterior ECG was done and showed no ST elevation, not even 0.5 The ECG normalized overnight.
Thus, this is BOTH an anterior and inferior STEMI in the setting of RBBB. How old is this antero-inferior STEMI? Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. the presence of such well developed, wide, anterior Q-wave suggests completed transmural STEMI. Could it be acute (vs.
Circulation, Volume 150, Issue Suppl_1 , Page A4147134-A4147134, November 12, 2024. Introduction:Elevated LDL cholesterol is linked to microvascular injury and adverse cardiac events in STEMI patients. This study examines the impact of prior statin use on LDL levels at the time of MI, focusing on NSTEMI and STEMI patients.
Echo on the day after admission showed EF of 30-35% and antero-apical wall akinesis with an LV thrombus [these frequently form in complete or near complete (no early reperfusion) anterior STEMI because of akinesis/stasis] 2 more days later, this was recorded: ST elevation is still present. Circulation 1999;99(15):1972-7.
COACT: The COACT trial was fatally flawed, and because of it, many cardiologists are convinced that if there are no STEMI criteria, the patient does not need to go to the cath lab. N Engl J Med [Internet] 2019;Available from: [link] Should all patients with shockable arrest be taken to angiography regardless of STEMI or No STEMI?
Circulation, Volume 150, Issue Suppl_1 , Page A4141319-A4141319, November 12, 2024. Background:The computational pressure-fluid dynamics applied to index of microcirculatory resistance, derived from coronary angiography (CPFD-caIMR) is a promising alternative method of IMR to evaluate the prognosis of STEMI patients.
This certainly looks like an anterior STEMI (proximal LAD occlusion), with STE and hyperacute T-waves (HATW) in V2-V6 and I and aVL. How do you explain the anterior STEMI(+)OMI immediately after ROSC evolving into posterior OMI 30 minutes later? This caused a type 2 anterior STEMI.
Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? Comments: STEMI with hypokalemia, especially with a long QT, puts the patient at very high risk of Torsades or Ventricular fibrillation (see many references, with abstracts, below). There is atrial fibrillation.
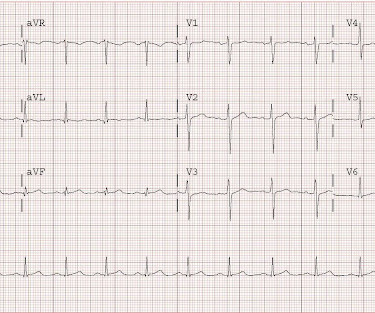
Despite the absence of significant coronary stenosis on her post-arrest cath — the ECG in Figure-1 is clearly diagnostic of an extensive anterolateral STEMI ( presumably from acute LAD [ L eft A nterior D escending ] coronary artery occlusion). The rhythm in ECG #1 is regular and supraventricular at a rate of ~75/minute.
This is a troponin I level that is almost exclusively seen in STEMI. So this is either a case of MINOCA, or a case of Type II STEMI. If the arrest had another etiology (such as old scar), and the ST elevation is due to severe shock, then it is a type II STEMI. I believe the latter (type II STEMI) is most likely.
Circulation: Cardiovascular Imaging, Ahead of Print. BACKGROUND:Microvascular obstruction (MVO) is associated with heart failure (HF) following ST-segmentelevation myocardial infarction.
Subtle as a STEMI." (i.e., Given that this is before it is released into the circulation by reperfusion therapy, this is a massively elevated troponin. In our study, there were 20/53 complete LAD OMI (TIMI-0 flow) which did not meet STEMI criteria. None of the 20 ever evolved to STEMI criteria. Hyperacute T-waves persist.
Circulation: Cardiovascular Imaging, Ahead of Print. BACKGROUND:T2-weighted imaging is commonly used to measure myocardial salvage in reperfused myocardial infarction but is hindered by poor reproducibility and indistinct boundaries. Early gadolinium enhancement (EGE) emerges as an alternative for measuring the area at risk.
STEMI MINOCA versus NSTEMI MINOCA STEMI occurs in the presence of transmural ischaemia due to transient or persistent complete occlusion of the infarct-related coronary artery. This has resulted in an under-representation of STEMI MINOCA patients in the literature. Circulation [Internet] 2017;135(16):1481–9. Circulation.
This is diagnostic of infero-posterior OMI, but it is falsely negative by STEMI criteria and with falsely negative posterior leads (though they do show mild ST elevation in V4R). They were less likely to have STEMI on ECG, and more likely to be initially diagnosed as non-ACS. Circulation 2007 2. Khan et al.
Recall from this post referencing this study that "reciprocal STD in aVL is highly sensitive for inferior OMI (far better than STEMI criteria) and excludes pericarditis, but is not specific for OMI." Circulation , 130 (25). Immediate versus delayed invasive intervention for non-stemi patients. The case continues. Mukherjee, D.,
Circulation: Cardiovascular Interventions, Ahead of Print. BACKGROUND:Patients with ST-segment–elevation myocardial infarction but no coronary microvascular injury are at low risk of early cardiovascular complications (ECC).
LVH and the diagnosis of STEMI - how should we apply the current guidelines? This one mimics inferior STEMI (Figure 4): Concentric LVH, NO wall motion abnormality Case 5. Contrast the above with this one, which has both LVH and inferior STEMI : There is limb lead LVH with superimposed inferior STEMI. They are quite rare.
It has been estimated that in the aggregate, they occur at a rate of about 3 per 1000 patients with acute MI, and most of these events occur in patients with STEMI. A mong patients with STEMI, ventricular septal rupture is the most common and free wall rupture is the least common.
By definition, this is a non-STEMI because there is not 1 mm of ST elevation in 2 consecutive leads. However, ST elevation is only an imperfect surrogate for complete acute persistent occlusion of an epicardial coronary artery without collateral circulation. It is neither fully sensitive nor specific.
The receiving emergency physician consulted with interventional cardiology who stated there was no STEMI. Is there STEMI? Circulation Research , 56 (2), 184–194. Circulation , 63 (2), 333–340. About one hour later his high sensitivity troponin I resulted at 3,000 ng/L (reference 3-54 ng/L). What is the rhythm? Moffat, M.
Step 1 to missing posterior MI is relying on the STEMI criteria. A prospective validation of STEMI criteria based on the first ED ECG found it was only 21% sensitive for Occlusion MI, and disproportionately missed inferoposterior OMI.[1] But it is still STEMI negative. A 15 lead ECG was done (below). In a study last year, 14.4%
This could facilitate the leakage of bacterial products into circulation and contribute to inflammation and adverse cardiac remodelling. Methods We examined 61 ST-elevation myocardial infarction (STEMI) patients who developed acute HF within 48 hours of successful percutaneous coronary intervention (PCI). to 264.65).
Note that they finally have laid to rest the new or presumably new LBBB as a criteria for STEMI. Note that they finally have laid to rest the new or presumably new LBBB as a criteria for STEMI. Also note that they allow ST depression c/w posterior MI to be a STEMI equivalent. Circulation 122:Abstract 101. Kurkciyan et al.
Circulation, Volume 150, Issue Suppl_1 , Page A4141170-A4141170, November 12, 2024. This study investigates the relationship between baseline 5-HTP levels and the incidence of major adverse cardiovascular events (MACE) in patients who have experienced ST-elevation myocardial infarction (STEMI).Objective:Our
The precordial ST-depression pattern on this ECG (and in this clinical setting) should immediately raise suspicion of Posterior STEMI! Posterior STEMI occurs in approximately 15-20% of acute MI, but the vast majority of the time it is seen in conjunction with inferior (Infero-Posterior) or lateral (Postero-Lateral) STEMI (1).
Precordial ST depression may be subendocardial ischemia or posterior STEMI. If you thought it might be a posterior STEMI, then you might have ordered a posterior ECG [change leads V4-V6 around to the back (V7-V9)]. So there was 3-vessel disease, but with an acute posterior STEMI. Circulation 2007;115(10):1306-24.
But because there was no new ST elevation, the ECG was signed off as “STEMI negative” and the patient waited to be seen. But the ECG still doesn’t meet STEMI criteria. It was therefore interpreted as “no STEMI” and the patient was treated with dual anti-platelets and referred to cardiology as “NSTEMI.” the cardiologist 5.
Circulation, Volume 150, Issue Suppl_1 , Page A4132742-A4132742, November 12, 2024. A random-effects model was used for outcomes with high heterogeneity.Results:We included 4 RCTs with 3173 patients comparing FFR-guided CR with culprit-only PCI in patients with STEMI and multivessel coronary artery diseases.
Circulation, Volume 150, Issue Suppl_1 , Page A4141279-A4141279, November 12, 2024. Background:Slow flow phenomenon is impaired coronary flow during percutaneous coronary intervention (PCI) in absence of mechanical obstruction, and it is associated with deteriorated outcome.
So they took the patient urgently to cath: 100% occlusion of inferior obtuse marginal branch of the circumflex, with collateral circulation. Had the cardiologists followed NSTEMI or transient STEMI guidelines, which recommend non-urgent cath, the patient could have redeveloped an OMI and had a worse outcome.
Barely any STE, and thus not meeting STEMI criteria. Annals of Emergency Medicine Cardiology was called to evaluate the patient immediately for emergent cath, but they stated that the ECG did not meet STEMI criteria and elected to wait for further information before proceeding with cath. He was given 6mg IV morphine for ongoing pain.
The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion. The patient in today’s case is a previously healthy 40-something male who contacted EMS due to acute onset crushing chest pain. The pain was 10/10 in intensity radiating bilaterally to the shoulders and also to the left arm and neck. The below ECG was recorded.
The "criteria" for posterior STEMI are 0.5 Is it STEMI or NonSTEMI? It was opened and stented with a door to balloon time of about 120 minutes (this is long for STEMI, but very short for a high risk Non STEMI). The 4th, after the opening of the artery and release of troponin from the cardiac circulation, was 99.9
Another overlooked OMI ( Cardiologist limited by STEMI Definition — OMI evident by Mirror Test ) — See My Comment at the bottom of the page in the September 21, 2020 post on Dr. Smith’s ECG Blog. Smith’s ECG Blog.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.















































Let's personalize your content