This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
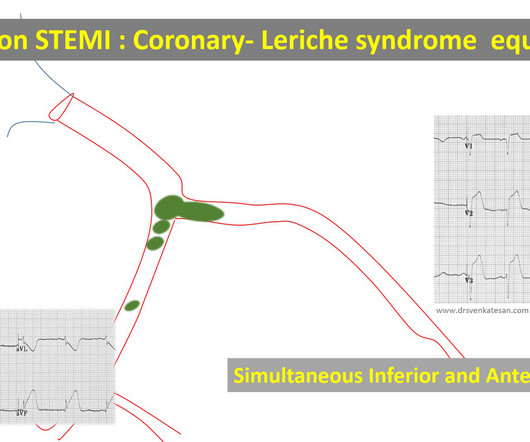
RCA-dependent LAD circulation through collaterals 3. True bifurcation STEMI with static thrombus (Carinal trapping of thrombus ,Coronary Lerish sydrome ) 4. Embolic STEMI with showers of emboli into both LCX and LAD Simultaneous or sequential Anterior and Inferior STEMI 5. Wrap around LAD true Global MI 2.
I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion. Non-STEMI guidelines call for “urgent/immediate invasive strategy is indicated in patients with NSTE-ACS who have refractory angina or hemodynamic or electrical instability,” regardless of ECG findings.[1]
Circulation, Volume 150, Issue Suppl_1 , Page A4142231-A4142231, November 12, 2024. Background:Little is known about the clinical relevance of interleukin (IL)-6 and the severity of patients with acute ST-elevation myocardial infarction (STEMI). All information about clinical and paraclinical parameters was recorded.
This is all suggestive of posterior STEMI, but not definitely diagnostic. mm in only one posterior lead is highly sensitive and specific for posterior STEMI). ST depression in V1-V4, isolated, may be either posterior STEMI or NSTEMI. A posterior ECG was done and showed no ST elevation, not even 0.5 The ECG normalized overnight.
Circulation, Volume 150, Issue Suppl_1 , Page A4147134-A4147134, November 12, 2024. Introduction:Elevated LDL cholesterol is linked to microvascular injury and adverse cardiac events in STEMI patients. This study examines the impact of prior statin use on LDL levels at the time of MI, focusing on NSTEMI and STEMI patients.
Echo on the day after admission showed EF of 30-35% and antero-apical wall akinesis with an LV thrombus [these frequently form in complete or near complete (no early reperfusion) anterior STEMI because of akinesis/stasis] 2 more days later, this was recorded: ST elevation is still present. Circulation 1999;99(15):1972-7.
This certainly looks like an anterior STEMI (proximal LAD occlusion), with STE and hyperacute T-waves (HATW) in V2-V6 and I and aVL. How do you explain the anterior STEMI(+)OMI immediately after ROSC evolving into posterior OMI 30 minutes later? This caused a type 2 anterior STEMI.
Despite the absence of significant coronary stenosis on her post-arrest cath — the ECG in Figure-1 is clearly diagnostic of an extensive anterolateral STEMI ( presumably from acute LAD [ L eft A nterior D escending ] coronary artery occlusion). The rhythm in ECG #1 is regular and supraventricular at a rate of ~75/minute.
This is a troponin I level that is almost exclusively seen in STEMI. So this is either a case of MINOCA, or a case of Type II STEMI. If the arrest had another etiology (such as old scar), and the ST elevation is due to severe shock, then it is a type II STEMI. I believe the latter (type II STEMI) is most likely.
Subtle as a STEMI." (i.e., Given that this is before it is released into the circulation by reperfusion therapy, this is a massively elevated troponin. In our study, there were 20/53 complete LAD OMI (TIMI-0 flow) which did not meet STEMI criteria. None of the 20 ever evolved to STEMI criteria. Hyperacute T-waves persist.
Circulation: Cardiovascular Imaging, Ahead of Print. BACKGROUND:Microvascular obstruction (MVO) is associated with heart failure (HF) following ST-segmentelevation myocardial infarction.
STEMI MINOCA versus NSTEMI MINOCA STEMI occurs in the presence of transmural ischaemia due to transient or persistent complete occlusion of the infarct-related coronary artery. This has resulted in an under-representation of STEMI MINOCA patients in the literature. Circulation [Internet] 2017;135(16):1481–9. Circulation.
This is diagnostic of infero-posterior OMI, but it is falsely negative by STEMI criteria and with falsely negative posterior leads (though they do show mild ST elevation in V4R). They were less likely to have STEMI on ECG, and more likely to be initially diagnosed as non-ACS. Circulation 2007 2. Khan et al.
LVH and the diagnosis of STEMI - how should we apply the current guidelines? This one mimics inferior STEMI (Figure 4): Concentric LVH, NO wall motion abnormality Case 5. Contrast the above with this one, which has both LVH and inferior STEMI : There is limb lead LVH with superimposed inferior STEMI. They are quite rare.
It has been estimated that in the aggregate, they occur at a rate of about 3 per 1000 patients with acute MI, and most of these events occur in patients with STEMI. A mong patients with STEMI, ventricular septal rupture is the most common and free wall rupture is the least common.
By definition, this is a non-STEMI because there is not 1 mm of ST elevation in 2 consecutive leads. However, ST elevation is only an imperfect surrogate for complete acute persistent occlusion of an epicardial coronary artery without collateral circulation. It is neither fully sensitive nor specific.
Step 1 to missing posterior MI is relying on the STEMI criteria. A prospective validation of STEMI criteria based on the first ED ECG found it was only 21% sensitive for Occlusion MI, and disproportionately missed inferoposterior OMI.[1] But it is still STEMI negative. A 15 lead ECG was done (below). In a study last year, 14.4%
This could facilitate the leakage of bacterial products into circulation and contribute to inflammation and adverse cardiac remodelling. Methods We examined 61 ST-elevation myocardial infarction (STEMI) patients who developed acute HF within 48 hours of successful percutaneous coronary intervention (PCI). to 264.65).
The precordial ST-depression pattern on this ECG (and in this clinical setting) should immediately raise suspicion of Posterior STEMI! Posterior STEMI occurs in approximately 15-20% of acute MI, but the vast majority of the time it is seen in conjunction with inferior (Infero-Posterior) or lateral (Postero-Lateral) STEMI (1).
Precordial ST depression may be subendocardial ischemia or posterior STEMI. If you thought it might be a posterior STEMI, then you might have ordered a posterior ECG [change leads V4-V6 around to the back (V7-V9)]. So there was 3-vessel disease, but with an acute posterior STEMI. Circulation 2007;115(10):1306-24.
But because there was no new ST elevation, the ECG was signed off as “STEMI negative” and the patient waited to be seen. But the ECG still doesn’t meet STEMI criteria. It was therefore interpreted as “no STEMI” and the patient was treated with dual anti-platelets and referred to cardiology as “NSTEMI.” the cardiologist 5.
Circulation, Volume 150, Issue Suppl_1 , Page A4141279-A4141279, November 12, 2024. Background:Slow flow phenomenon is impaired coronary flow during percutaneous coronary intervention (PCI) in absence of mechanical obstruction, and it is associated with deteriorated outcome.
Barely any STE, and thus not meeting STEMI criteria. Annals of Emergency Medicine Cardiology was called to evaluate the patient immediately for emergent cath, but they stated that the ECG did not meet STEMI criteria and elected to wait for further information before proceeding with cath. He was given 6mg IV morphine for ongoing pain.
The "criteria" for posterior STEMI are 0.5 Is it STEMI or NonSTEMI? It was opened and stented with a door to balloon time of about 120 minutes (this is long for STEMI, but very short for a high risk Non STEMI). The 4th, after the opening of the artery and release of troponin from the cardiac circulation, was 99.9
Another overlooked OMI ( Cardiologist limited by STEMI Definition — OMI evident by Mirror Test ) — See My Comment at the bottom of the page in the September 21, 2020 post on Dr. Smith’s ECG Blog. Smith’s ECG Blog.
“ Since Intravenous lysis looks too simplistic, that do not need expertise, and lacks a commercial trail, it is wrongly depicted as inferior management strategy in STEMI “ Every one of us is equally responsible for this sorry state of affairs. In LAD STEMI time is more crucial. Circulation 2005;111:761-7.
This blog post reviews the basics for predicting the " C ulprit" A rtery — as well as the importance of the term, " O MI" ( = O cclusion-based MI ) as an improvement from the outdated STEMI paradigm. ECG Blog #294 — How to tell IF the "culprit" artery has reperfused. ECG Blog #194 — AIVR as a sign that the "culprit" artery has reperfused.
Circulation, Volume 150, Issue Suppl_1 , Page A4140882-A4140882, November 12, 2024. Patients with documented STEMI, left ventricular thrombus, mechanical mitral or aortic valve replacement were excluded. Introduction:Atrial fibrillation (A fib) is the most common arrhythmia affecting 1-2% of the general population.
You've read in my previous posts that I have a lot of evidence that Wellens' represents spontaneously reperfused STEMI in which the STEMI went unrecorded. New ST elevation diagnostic of STEMI [equation value = 25.3 Circulation 1991;84:1454-1455. This T-wave inversion morphology is very specific for Wellens' waves.
Circulation, Volume 150, Issue Suppl_1 , Page A4147397-A4147397, November 12, 2024. Background:Ischemic heart disease (IHD) is a prevalent cardiovascular disease (CVD) associated with high morbidity and mortality. Over 600,000 percutaneous coronary interventions (PCI) are performed each year for IHD.
Is primary PCI superior to thrombolysis in the first hour of STEMI ? Circulation. No, it is not. I know, most interventional cardiologists cannot accept this fact and would strongly disagree. Still, they know very well there is no clear data to back up their belief. 2003 Dec 9;108(23):2851-6. doi: 10.1161/01.CIR.0000103122.10021.F2.
Circulation, Volume 150, Issue Suppl_1 , Page A4125093-A4125093, November 12, 2024. Types of ACS include stable angina 5.3% (n=8), unstable angina 24% (n=36), NSTEMI 28.7% (n=43), and STEMI 24% (n=36). Introduction:Inflammation plays an important role in the pathogenesis of coronary artery disease and Acute Coronary Syndrome (ACS).
Circulation, Volume 150, Issue Suppl_1 , Page A4122543-A4122543, November 12, 2024. Background:Ticagrelor has been reported to cause shortness of breath (SOB) in 6 to 9 % of patients. Precise mechanisms are not enirely understood. The patient received ticagrelor in loading dose followed by 90 mg b.i.d plus low-dose aspirin.
The patient was brought to the ED as a possible Code STEMI and was seen directly by cardiology. Similarly, STEMI guidelines call for urgent angiography for refractory ischemia or electrical/hemodynamic instability, regardless of ECG findings. On arrival, GCS was 13 and the patient complained of ongoing chest pain.
Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. He does have a recently diagnosed PE, and has not been taking his anticoagulation due to cost. He had a previous ECG on file: Proving the findings are new The cath lab was activated. He was given aspirin and sublingual nitro and the pain resolved.
STEMI MINOCA versus NSTEMI MINOCA STEMI occurs in the presence of transmural ischaemia due to transient or persistent complete occlusion of the infarct-related coronary artery. This has resulted in an under-representation of STEMI MINOCA patients in the literature. Circulation [Internet] 2017;135(16):1481–9. Circulation.
The role of collateral circulation in CTO that can compensate even during exercise is well known at patient level data. One more remote risk in CTO is, acute collateral shutdown causing STEMI/NSTEMI. (DECISION-CTO,EURO-CTO,EXPLORE,IMPACTOR) Opening a CTO, for reasons other than angina (i.e.
As per Dr. Aslanger — a number of medical providers were initial confused by what initially appears as marked ST elevation with reciprocal ST depression, indicative of an acute STEMI. That was also my initial concern. No "baseline" ECG is available for comparison.
Later, I found old ECGs: 5 month prior in clinic: V5 and V6 look like OMI 9 months prior in clinic with no chest symptoms: V5 and V6 look like OMI 1 year prior in the ED with chest pain: V5 and V6 sure look like a STEMI For this ECG and chest pain in the ED, the Cath lab activated. But the angiogram was clean. There was no OMI.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.















































Let's personalize your content