This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
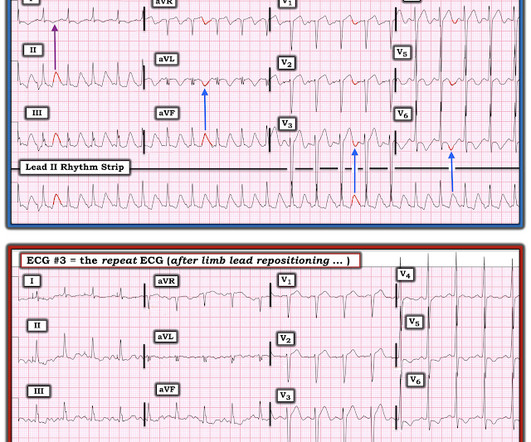
DISCUSSION: The 12-lead EKG EMS initially obtained for this patient showed severe ischemia, with profound "infero-lateral" ST depression and reciprocal ST elevation in lead aVR. The ECG cannot diagnose the etiology of ischemia; it only the presence of ischemia, from whatever etiology.
Incredibly , this case was just published in Circulation on January 22, 2018 (thanks to Brooks Walsh for finding this!) link] Circulation. Originally published January 22, 2018 Here is a case from Circulation year 2000 that was misdiagnosed as due to pancreatitis. Journal of Electrocardiology. 2012;45(1):15-17. 2010.12.162.
It is interesting to note, while plasminogen levels are elevated, D-dimer is also increased, indicating an ongoing fight between pro & anticoagulant forces, converting the physiological maternal- placental bed a mini harmless DIC equivalent zone. The list is increasing in a steady fashion. What does it imply ?
If you still have not read it, I strongly recommend that you read the following article on the diagnosis of "posterior" MI: Ischemic ST-Segment Depression Maximal in V1-V4 (Versus V5-V6) of Any Amplitude Is Specific for Occlusion Myocardial Infarction (Versus Nonocclusive Ischemia), by Meyers HP et al. Circulation 2002; 105(4): 539-42.
6 This novel study marks a significant milestone in the field, evaluating the effectiveness of FFR CT in detecting ischemia-producing coronary stenosis in patients with severe PAD. Diagnosis and treatment of ischemia-producing coronary stenoses improves 5-year survival of patients undergoing major vascular surgery.” Circulation, vol.
Extensive conduction system abnormalities can have various causes (ischemia, genetic, infectious, amyloid, etc). The physiologic reason for this — is thought to be the result of momentarily increased circulation from mechanical contraction arising from the "sandwiched in" QRS complex. The QRS complex in ECG #1 is wide.
We wish, our understanding about cardiac contractile physiology is deep and nearly complete. The simple reason could be we can address the ischemia a potential arrhythmic target by some form of revascularization in IDCM. Circulation. The second reason is, NDCM is a progressive primary muscle disease. 2022 Feb 8;145(6):427-436.
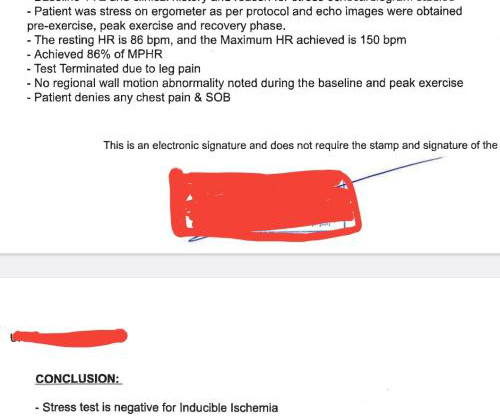
We know, stress tests can give false positive results suggesting ischemia in at least 20% of patients for various reasons. Final message Most of us (Cardiologists) find it difficult to trust physiology, ie excercise capcity. Though, we eloborately debate about physiology-based intervention in every conference.
Evidence of acute ischemia (may be subtle) vii. ST segment and T wave abnormalities consistent with or possibly related to myocardial ischemia. Fourth, syncope in the elderly often results from polypharmacy and abnormal physiologic responses to daily events. Circulation. Left BBB vi. Pathologic Q-waves viii. LVH or RV d.
It is possible there is microvascular dysfunction producing residual transmural ischemia. But this is most common when there is prolonged ischemia, and this patient had the fastest reperfusion imaginable! Circulation Research , 114 (12), 18521866. Circulation , 92 (3), 657671. Circulation , 125 (3), 491496.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.















Let's personalize your content