This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
BackgroundPlaque progression (PP) is critical between subclinical atherosclerosis and plaque rupture. Small dense lowdensity lipoprotein cholesterol (sdLDLC) is considered as the most atherogenic lipoprotein. Journal of the American Heart Association, Ahead of Print.
We used carotid ultrasounds to detect plaque at baseline and follow‐up in 2006 to 2009 (median follow‐up=5.5 had low‐density lipoprotein cholesterol ≥160 mg/dL, which is higher than the recommended threshold for lifestyle or medical interventions in young adults of 20 to 39 years old. Lipids were measured after a 12‐hour fast.
You cannot eliminate the plaque entirely, but multiple clinical trials have shown plaque regression using high-intensity cholesterol-lowering treatments, which I have discussed previously. All of these parameters are important and need to be considered when evaluating plaque regression. REVERSAL Investigators.
BACKGROUND:Small dense low-density lipoprotein cholesterol (sdLDL-C) particles are more atherogenic than large and intermediate low-density lipoprotein cholesterol (LDL-C) subfractions. Incident carotid plaques and their vulnerability were detected by carotid ultrasound at follow-up (2021). Stroke, Ahead of Print.
Carotid ultrasound results were divided into two groups based on the presence or absence of plaque. Carotid plaque was observed in 1140 (43.5%) subjects and CACS>0 in 1172 (44.7%) subjects. Lp(a) levels were categorized into two groups: below 50 mg/dl and 50 mg/dl or higher. 1692 (64.6%) were male.
The primary outcome was the prevalence of carotid artery plaques assessed by ultrasound. Secondary outcomes included changes in NMR-derived lipoprotein subclasses and their mediation effects on carotid plaque. Fish oil supplementation was significantly associated with reduced prevalence of carotid plaques (P=0.023).
Plaque regression can be demonstrated by ultrasound evaluation of the carotids which are easily accessible. High density lipoprotein cholesterol in the blood increases with regular exercise. HDL is involved in reverse cholesterol transport from the blood vessels to the liver.
Cholesterol levels go up when thyroid function comes down. This in turn can enhance the chance of plaque build-up in the blood vessels of the heart (coronary arteries). Ultrasound image of the heart – echocardiogram, showing fluid collection around the heart, marked as PE, short for pericardial effusion.
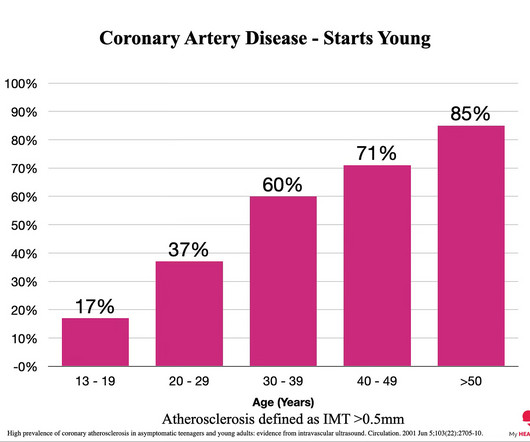
Everyone starts with no plaque in the coronary arteries, but over a long enough time frame, everyone develops plaque in their coronary arteries. By age 80, almost everyone will have evidence of advanced plaque in their coronary arteries, as defined by a cardiac CT 1. Plaque accumulation happens in stages. You got it.
Echocardiography – We can use ultrasound to visualize the heart and look at how well it pumps. With time, fat and cholesterol can get trapped in the areas of wear and tear and cause plaque formation. The plaques can damage us in 2 ways. This is termed as diastolic dysfunction.
Heart disease, the build-up of plaque in the coronary arteries, typically starts years, if not decades, prior to an event. These noninvasive scans look directly at the coronary arteries rather than assessing for the risk factors for coronary artery disease eg LDL cholesterol, high blood pressure etc. As the line goes, “No Plaque.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












Let's personalize your content