This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Genes influence various biological processes, including cholesterol metabolism, blood pressure regulation, and the strength and structure of your heart and blood vessels. Specific genetic variants, such as those affecting cholesterol metabolism, can increase the likelihood of plaque buildup in the arteries. How Do Genetic Factors Work?
These cases are particularly challenging because traditional prevention strategies, which target known risks like high LDL cholesterol, hypertension, diabetes, and smoking, may not apply. Enhancing Adherence: Simplify treatment plans and build trust through patient education.
The 14 Factors Include: Hearing Loss High LDL cholesterol Less Education Traumatic Brain Injury Depression Social Isolation Hypertension Obesity Smoking Excess Alcohol Diabetes Physical Inactivity Air Pollution Visual Loss Dementia prevention, intervention, and care: 2024 report of the Lancet standing Commission When You Intervene Matters.
had low‐density lipoprotein cholesterol ≥160 mg/dL, which is higher than the recommended threshold for lifestyle or medical interventions in young adults of 20 to 39 years old. Baseline dyslipidemia prevalence was 55.2%, 73.6%, and 78.0% for participants 15 to 19, 20 to 29, and 30 to 39 years old, respectively. Approximately 2.8%
Newly included risk factors— untreated vision loss and high LDL cholesterol —underscore the critical role of these elements in maintaining cognitive health. The Cholesterol Connection Cholesterol’s recognition as a risk factor for dementia marks a pivotal advancement in understanding, preventing, and delaying cognitive decline.
Cardiovascular risk factors were measured at 1‐year intervals for 4 years in 4249 adults with overweight or obesity and type 2 diabetes who were randomly assigned to ILI or diabetes support and education. to −0.59]), total cholesterol (β=−1.12 [95% CI, −1.75 to −0.48]), and low‐density lipoprotein cholesterol (β=−1.04 [95% CI, −1.59
The AHA strives to further understand and help heal health problems inflicted by structural racism, a public health crisis that can significantly damage physical and mental health and perpetuate disparities in access to health care, education, income, housing, and several other factors vital to healthy lives.
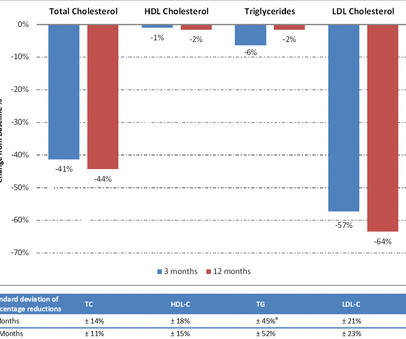
Referred patients are assessed for eligibility and given tailored, person-centred support, education and monitoring to promote treatment adherence and lipids optimisation. Mean total cholesterol decreased from 7.7±1.6 mmol/L at 3 months (41% reduction), while mean low-density lipoprotein-cholesterol (LDL-C) fell from 5.0±1.6
Individuals with LVH were older, more likely to have hypertension, diabetes, known cardiovascular disease (CVD) and elevated levels of cholesterol and creatinine. Further, they were more likely to be of African descent (Creole) and have lower educational level. to 1.83)), low educational level (1.49 (1.28
10kg) Out of which just 250 mg of cholesterol is streaming in blood. We must understand Fat, lipid and cholesterol are different entities. While the total body seems to do little in determining cholesterol levels, what is more scientifically shocking is slope of the curve between blood LDL levels and plaque burden is rarely linear.
He added, “I think most people think of obesity and being out of shape as the primary cause of heart attacks, but we clearly have shown that high cholesterol and blood pressure, which are often heavily influenced by genetics, are the primary risk factors.” “We
It typically includes supervised exercise training, heart-healthy living education, stress reduction counseling and nutrition guidance. The program provides education and support for controlling blood pressure, managing cholesterol levels, maintaining a healthy weight and quitting smoking.
Risk factors for PAD include smoking; having Type 1 or Type 2 diabetes, high blood pressure, high cholesterol, chronic kidney disease, atherosclerosis in other parts of the body (such as coronary artery disease); and being age 75 years or older. and Global Data From the American Heart Association. Black adults with PAD in the U.S.
Patients received access to a bespoke web-based platform and were invited to attend weekly, online group-based supervised exercise sessions and educational workshops. To support self-management, patients were provided with a Fitbit, a home blood pressure (BP) monitor and an interactive workbook. kg, p<0.001). p<0.001).
VA sites work with an AHA QI consultant to develop and deploy a local quality improvement plan to help overcome site specific barriers preventing Veterans from achieving optimal cholesterol levels. In conclusion, this initiative led to target LDL levels in 39% of patients which represents a significant population.
Albumin, B12, total bilirubin, cholesterol, CRP, ferritin, iron, folate, hbA1c, HDL, LDL, hemoglobin, MCV, INR, ALT, triglycerides, and vitamin D were abstracted from health records. Patients were divided into underweight, normal weight, overweight, and obese according to World Health Organization BMI criteria. 5.94) groups.
It further noted this is intended to help physicians personalize treatment for conditions such as hypertension and high cholesterol, or prevent them entirely. Mayo Clinic will use any revenue it receives to support its not-for-profit mission in patient care, education and research.
23, 2024 – The Society for Vascular Surgery (SVS) is launching a three-year patient education campaign, Highway to Health, to empower Americans to learn their SVS Strong Vessel Score and start a conversation with their doctor to see if a vascular surgeon could be a good addition to their overall care team.
The independent variable or “exposure” was the LE8 score, which was based on data on blood pressure, blood glucose and cholesterol, body mass index, smoking, physical activity, sleep duration and diet. Participants with prior stroke, transient ischemic attack (TIA) or myocardial infarction (MI) were excluded.
Key secondary and exploratory outcomes include improvement in a composite cardiovascular health metric, CR engagement, quality of life, health factors (including low‐density lipoprotein‐cholesterol, hemoglobin A1c, weight, diet, smoking cessation, blood pressure), and psychosocial factors.
One of my colleagues was joking ,nowadays patients force us to read or even educate us. There you go, into the perils of hyper- education of modern society. After all, please remember much greater men like Abraham Lincoln and Mahatma Gandhi lived a stellar life , in the grand old era when no one knew what was cholesterol and lipids.”
Using digital cardiac care tools resulted in an increase considering their positive role in monitoring health through: Smoking cessation Weight loss programs Optimised blood pressure control Glycemic control in diabetes Lipid and cholesterol levels Recommended Read: Medical Imaging Emerging Trends in 2021 2.
Brad notes that his primary care physician told him he was young, fit, and had a low bad cholesterol (LDL) and needed a calcium scan rather than a heart flow scan. Subscribe for free to receive new posts and support my work. Question 1. Does Brad need a calcium scan?
A key opinion leader can be critically important in helping to educate physicians about a new drug. Try publishing a paper suggesting that cholesterol lowering is a waste of time, when the market for cholesterol lowering drugs is worth hundreds of billions.
Background:Lower educational attainment (EA) and smaller social network are each associated with a greater risk for incident stroke. In fully adjusted models, Mexican-American ethnicity, diabetes, and high cholesterol were associated with higher recurrence. Stroke, Volume 56, Issue Suppl_1 , Page ATP276-ATP276, February 1, 2025.
mg tablets), together with Caristo Diagnostics , a leading cardiac disease diagnostics company with the novel CaRi-Heart technology to visualize and quantify coronary inflammation, announced today their collaboration to improve awareness and clinical education about the central role of inflammation in coronary artery disease.
Model covariates included sex, age, marital status, household size, household income, education, race/ethnicity, insurance, body mass index (BMI), and an indicator of the condition of interest. SD=1.5), high cholesterol (-5.7, SD=1.5), high cholesterol (-5.7, SD=21.8), followed by other (i.e., SD=21.0), Hispanics (59.3,
ICVH can be depicted vis-a-vis the seven metrics of the AHA: blood pressure levels, total cholesterol and glucose levels, smoking status, body mass index, physical activity levels, and dietary intake through the consumption of fruits and vegetables. Data were obtained from the Life Stage Food and Nutrition Surveillance Survey (VIANEV).
When adjusted for age, sex, race/ethnicity, education and PIR, the mean LE8 score was significantly lower in those who reported a history of stroke at (59.2, 95% CI, 57.8-60.5) compared to those who did not (63.8, 95% CI, 63.4-64.2) in those who did not.
When adjusted for age, sex, race/ethnicity, education and PIR, the mean LE8 score was significantly lower in those who reported a history of stroke at (59.2, 95% CI, 57.8-60.5) compared to those who did not (63.8, 95% CI, 63.4-64.2) in those who did not.
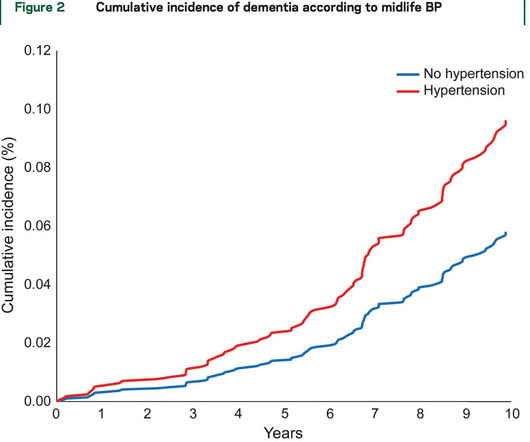
Education‐adjusted cut points were used to define suspected MCI. 1.38]) was also significantly associated with suspected MCI, after adjusting for age, sex, education level, mean arterial pressure, hypertension, diabetes, low‐density lipoprotein cholesterol, and smoking status. men; age range, 35–96 years [mean±SD, 59.9±11.8 years])
The model adjusted for age, sex, body mass index, smoking, hypertension, diabetes, low‐density lipoprotein cholesterol, estimated glomerular filtration rate, education, and physical activity at baseline. We first identified baseline lipid species associated with risk of CHD, followed by replication in a European population.
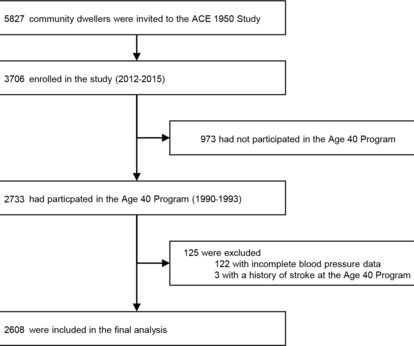
We categorised participants by systolic blood pressure (SBP) at age 40 (<120 mm Hg (reference), 120–129 mm Hg, 130–139 mm Hg and ≥140 mm Hg) and compared stroke risk using Cox proportional hazard regressions adjusted for age, sex, smoking, cholesterol, physical activity, obesity and education.
Socioeconomic status (SES) was measured on the basis of income and education. Targeted interventions reducing the prevalence of smoking, diabetes, hypertension, and high cholesterol in patients with low SES could mitigate these disparities.
Lower income, education, occupation (non‐management/professional versus management/professional occupations), and insurance status (uninsured, Medicaid, Veterans Affairs, or Medicare versus private insurance) were associated with lower CVH scores (allP<0.01). Heterogeneity by sex was assessed. Participants had a mean age of 54.8 years
BackgroundHigher scores for the American Heart Association Life's Essential 8 (LE8) metrics, blood pressure, cholesterol, glucose, body mass index, physical activity, smoking, sleep, and diet, are associated with lower risk of chronic disease.
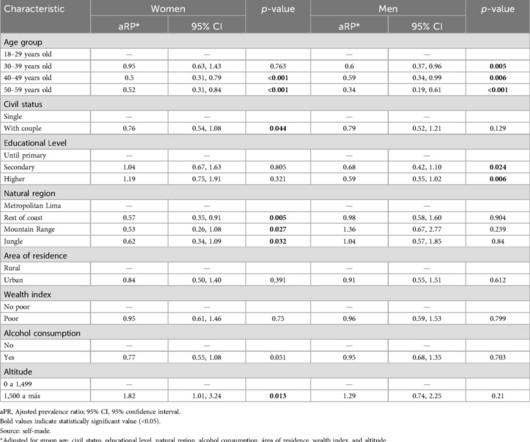
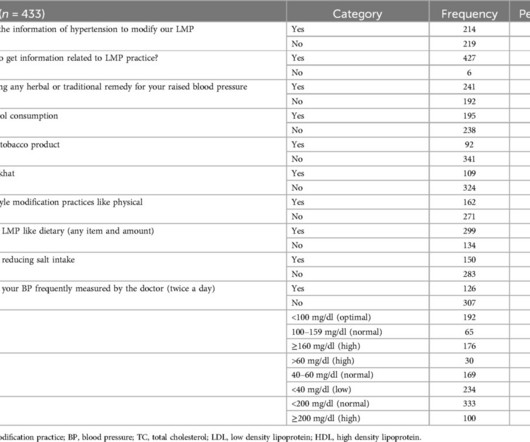
Alcohol consumption (AOR=0.64, 95% CI: 0.420.96), ever-practiced reducing salt intake (AOR=2.48, 95% CI: 1.573.93), and low-density lipoprotein cholesterol levels in the blood (>160mg/dl) (AOR=3.3, Of the total participants, 56.1% (95% CI, 51.3860.74) of the patients practiced the recommended lifestyle modifications.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.































Let's personalize your content