This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
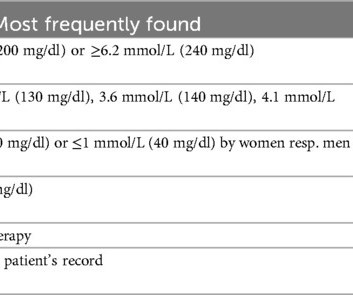
Dyslipidemia is extensively analyzed in clinical trials investigating its role as a risk factor for coronaryarterydisease (CAD). However, its definition varies vastly among studies, leading to different attributions to the variable dyslipidemia.
Reversing or regressing coronaryarterydisease is possible. You cannot eliminate the plaque entirely, but multiple clinical trials have shown plaque regression using high-intensity cholesterol-lowering treatments, which I have discussed previously. Subscribe now 1 Pathophysiology of CoronaryArteryDisease.
BackgroundLow-Density Lipoprotein Cholesterol (LDL-C) is the primary lipid therapy target for coronaryarterydisease (CAD) patients after percutaneous coronary intervention (PCI). Employing Multivariate Cox regression analysis, we assessed the correlation between RLP-C and NTLs progression.
The Lundquist Institute for Biomedical Innovation at Harbor-UCLA Medical Center, in collaboration with researchers across multiple institutions, has published a new study that challenges the long-held belief that high cholesterol correlates and even directly causes coronaryarterydisease, or plaque buildup in the arteries in metabolically healthy (..)
Background The purpose of this study was to evaluate the relationship between remnant cholesterol (RC) to high-density lipoprotein cholesterol (HDL-C) ratio and the risk of coronaryarterydisease (CAD).
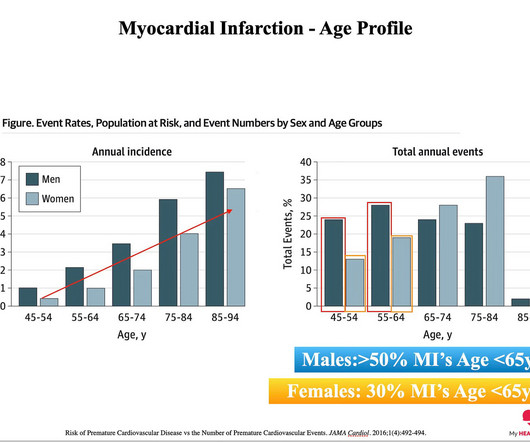
A novel molecular pathway to explain how a mutation in the gene ACTA2 can cause individuals in their 30s -- with normal cholesterol levels and no other risk factors -- to develop coronaryarterydisease has now been identified,
Introduction Studies in cholesterol-fed rabbits showed that anti-proliferative chemotherapeutic agents such as paclitaxel associated with solid lipid nanoparticles (LDE) have marked anti-atherosclerotic effects. In addition, association with LDE nearly abolishes paclitaxel toxicity.
BACKGROUND:Genome-wide association studies identified a 20-Kb region of chromosome 8 (8q24.13) associated with plasma lipids, hepatic steatosis, and risk for coronaryarterydisease. Circulation: Genomic and Precision Medicine, Volume 17, Issue 6 , Page e004674, December 1, 2024. locus to these traits. locus to these traits.
Background Coronaryarterydisease (CAD) is one of the most prevalent cardiovascular diseases where serum lipoprotein oxidation plays a significant role. Results CAD subjects had higher oxHDL/HDL cholesterol (HDL-c) ratio [0.102 (0.0920.112) vs. 0.080 (0.0700.090), P=0.004] and oxLDL/LDL cholesterol (LDL-c) ratio [129.2
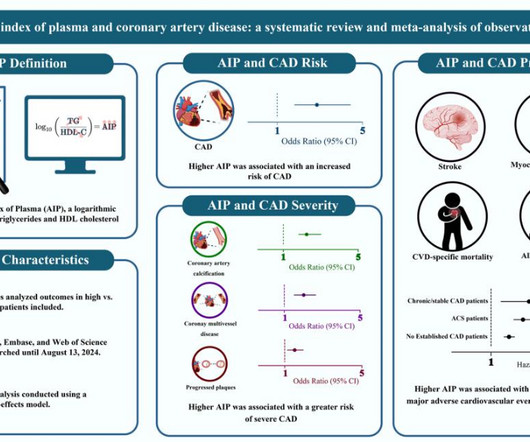
Atherogenic index of plasma (AIP), a novel logarithmic index that combines fasting triglyceride and high-density lipoprotein cholesterol concentrations, is associated with the burden of atherosclerosis.
Small dense lowdensity lipoprotein cholesterol (sdLDLC) is considered as the most atherogenic lipoprotein. Journal of the American Heart Association, Ahead of Print. BackgroundPlaque progression (PP) is critical between subclinical atherosclerosis and plaque rupture.
Background The SYNTAX score is a score that grades the severity and complexity of coronary lesions. In this study, we aimed to investigate the relationship between triglyceride/high-density lipoprotein cholesterol (triglyceride/HDL-C) ratio and SYNTAX scores in patients presenting with non-ST elevation myocardial infarction (NSTEMI).
Our objective was to assess whether metformin could mitigate statin-induced adverse effects on PCSK9, thereby improving lipid profiles in patients with coronaryarterydisease (CAD) but without diabetes.
Do you use advanced cholesterol testing? This is all about understanding whether a 'risk factor,’ e.g. High LDL-C cholesterol, has translated into significant ‘disease,’ e.g. coronaryarterydisease. In general, the more of the disease, the higher the risk. eg ApoB, Lp(a) etc.
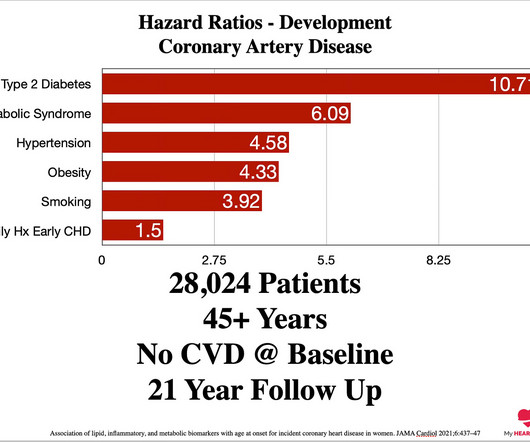
mmol/l (130 mg/dl) or below, between 20-50% will already have coronaryarterydisease. As HBA1c increases, even in the normal range, the probability of coronaryarterydisease increases. For HBA1c, the trend is similar. Remember, these are all in the ‘normal’ range. How LONG has it been abnormal?
Recent clinical trials demonstrated that proprotein convertase subtilisin/kexin 9 (PCSK9) inhibitors reduce cardiovascular events without affecting systemic inflammation in the patients with coronaryarterydisease, as determined by high sensitivity C-reactive protein (CRP) levels.
Atherosclerotic coronaryarterydisease (CAD) is the causal pathological process driving most major adverse cardiovascular events (MACE) worldwide. For many disease areas, nearly a half of drugs are approved by the U.S. Food & Drug Administration based on beneficial effects on surrogate endpoints.
This cohort study investigates the association between very high high-density lipoprotein cholesterol (HDL-C) level and outcomes in patients with coronaryarterydisease.
Importantly, all of the participants had recently undergone percutaneous coronary intervention (PCI) — a surgical procedure in which a stent is placed in a coronaryartery to open up a blockage. All of the participants had stable coronaryarterydisease and were on lipid-lowering therapies during the study.
Background Lipoprotein(a) [Lp(a)] is an independent, causal risk factor for cardiovascular disease. However, it is still unclear whether controlling low-density lipoprotein cholesterol (LDL-C) to optimal levels can attenuate cardiovascular risk mediated by elevated Lp(a), especially in the setting of secondary prevention.
Every lipoprotein particle has one APO B protein. ( **Please note the B ) When we measure APO B levels, this is what we are measuring to give an estimate of the number of cholesterol particles and the subsequent risk of cardiovascular disease. APO E is also centrally involved in cholesterol metabolism. Here’s how.
BackgroundIn the SPARCL (Stroke Prevention by Aggressive Reduction in Cholesterol Levels) trial, atorvastatin (80 mg per day) was compared with placebo in patients with recent stroke or transient ischemic attack and no known coronaryarterydisease. Journal of the American Heart Association, Ahead of Print.
I do apologise for being direct, but this issue is one of the most frequent barriers I encounter to initiating cholesterol-lowering therapy. At the exact same time, cholesterol concentrations are also at their lowest. At the exact same time, cholesterol concentrations are also at their lowest. Let’s break this down.
An elevated Lp(a) is the most common genetic cholesterol disorder impacting 10-20% of the population. Everyone should have an Lp(a) blood test at least once, but this is an absolutely must-do test if you have an early family history of heart disease. The trial is fully enrolled, but results are still likely several years away.
Background and aims Epidemiology of atherosclerotic cardiovascular disease might be different in patients with polygenic hypercholesterolemia plus high levels (≥30 mg/dl) of Lp(a) (H-Lpa) than in those with polygenic hypercholesterolemia alone (H-LDL). The median duration of follow-up was 10 years (IQR 3–16). 3.17, P = 0.006).
The identification of a variant in theHDAC9gene as a risk factor for large-artery atherosclerotic stroke, and subsequently coronaryarterydisease, has opened novel treatment pathways for stroke and more widely atherosclerotic disease. Stroke, Volume 54, Issue 12 , Page 3182-3189, December 1, 2023.
Background:Lipoprotein a (Lp(a)) is known to be associated with coronaryarterydisease and carotid artery atherosclerosis. This association remains independent even after adjustment for factors such as statin use or low-density lipoprotein cholesterol (LDL-C) levels.
An elevated Lp(a) is a common genetic factor that is independently and causally related to premature coronaryarterydisease. The occurrence of disease in this instance is probabilistic, not deterministic. An elevated Lp(a) does increase the risk of early cardiovascular disease, but that risk is not set in stone.
High blood pressure – Hypertension is a significant risk factor for heart disease. High cholesterol levels – Elevated levels of bad cholesterol can contribute to plaque buildup in your arteries, increasing the risk of heart disease. Smoking – Smoking is the most preventable cause of heart disease.
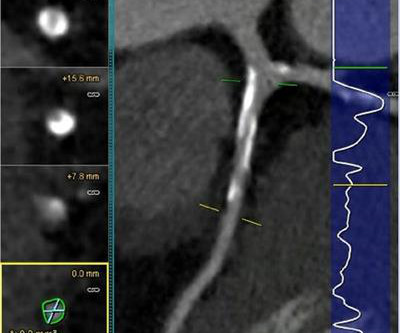
Understanding your Cholesterol Blood Test Panel. Lifestyle Approaches To Preventing Heart Disease. Understanding the role of Cardiac CT in assessing coronaryarterydisease. How to use lifestyle measures to reverse coronaryarterydisease. The Role Of Insulin Resistance.
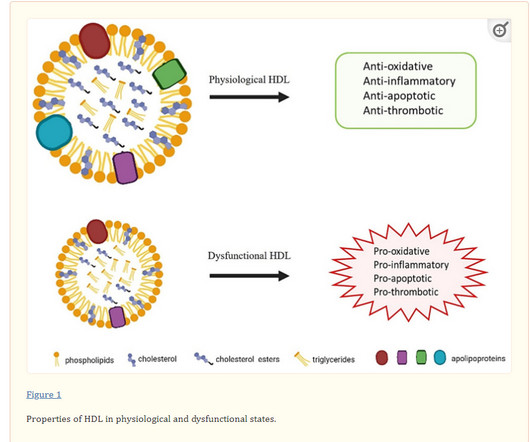
(Article will be linked) We know ,HDL carries free cholesterol from peripheral cells, including macrophages and endothelial cells. This is the much famous Reverse Cholesterol Transport(RCT) and the anti-atherosclerotic effect of HDL.It Lipids in Cardiovascular Disease Eduardo Z. HDL : The untold story ! Cardiovasc.
The results showed that compared with the control group, PCSK9 inhibitors significantly reduced low-density lipoprotein cholesterol (WMD=1.24mmol/L, 95% confidence interval (CI): 1.28 to 1.20), total cholesterol, triglycerides, and Lp(a) levels while increasing high-density lipoprotein cholesterol levels.
To induce atherosclerosis, mice were fed high fat diet (HFD) for 6 weeks following partial ligation of left carotid artery in C57BL6 mice. Additionally, DAPTA reduced the migratory potential, reduced cholesterol uptake and improved the functionality (suppression of T cell) of M-MDSCs. 3ng/day for 15 days).M-MDSCs
Albumin, B12, total bilirubin, cholesterol, CRP, ferritin, iron, folate, hbA1c, HDL, LDL, hemoglobin, MCV, INR, ALT, triglycerides, and vitamin D were abstracted from health records. Patients were divided into underweight, normal weight, overweight, and obese according to World Health Organization BMI criteria. 5.94) groups.
Non-HDL Cholesterol There is no ‘Good’ cholesterol on a standard cholesterol blood test. There really is only bad cholesterol. The relationship is simple—higher cholesterol for longer increases your risk of coronaryarterydisease 4. What is your Non-HDL cholesterol?
Genes influence various biological processes, including cholesterol metabolism, blood pressure regulation, and the strength and structure of your heart and blood vessels. A family history of heart disease often indicates that genetic factors might be at play. Mutations can lead to elevated LDL (bad cholesterol) levels.
mg reduces the risk of major adverse cardiovascular events (MACE) and supports its use in the treatment of cardiovascular disease. mg improved several measures of plaque volume changes over a period of 12 months in patients with stable coronaryarterydisease, Dr. Budoff continued.
The fundamental cause of atherosclerosis is when a cholesterol particle crosses into the artery wall from the bloodstream, gets stuck, and sets off an inflammatory process 1. ApoB particles crossing the artery wall to cause Atherosclerosis. Every cholesterol particle has a protein marker called ApoB on its outside.
Heart Valve Disease If one or more heart valves are not functioning correctly, it can cause blood to flow backward, putting extra pressure on the heart, which may cause it to expand to compensate for the inefficiency. Monitor blood pressure and cholesterol levels regularly. Avoid smoking and limit alcohol intake.
Coronaryarterydisease is caused by the retention of a cholesterol particle in the artery wall. But if a retained cholesterol particle is the spark. Insulin resistance and diabetes may not ‘ cause ’ coronaryarterydisease, but they are huge accelerants. Timing Matters.
Plaques that build up in the heart’s arteries contain fats, cholesterol and other substances; most heart attacks and serious cardiac events occur when pieces of such plaques break off and travel through the blood vessel, causing a blockage. Patients were 64 years old, on average.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






































Let's personalize your content