This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
He did not remember whether he had experienced any chestpain. This is a critically important determination because of the 2017 AHA/ACC/HRS Guidelines for Management of Patients with Ventricular Arrhythmias and the Prevention of SuddenCardiacDeath. However, he did not remember much from the day of the arrest.
Unlike a heart attack, cardiac arrest is an electrical malfunction that causes the heart to stop beating suddenly. Without immediate intervention, suddencardiacdeath can occur within minutes. Without prompt treatment, parts of the heart muscle may become damaged or die.
No prior exertional complaints of chestpain, dizziness, lightheadedness, or undue shortness of breath. No family history of suddencardiacdeath, cardiomyopathy, premature CAD, or other cardiac issues. He denied headache or neck pain associated with exertion. No similar symptoms in the past.
Clinical contexts leading to diagnosis were SCD in 3 (6%), ventricular arrhythmias in 15 (29%), chestpain in 8 (15%), heart failure in 6 (12%) and familial screening in 20 (38%). Significant right ventricular involvement was an exclusion criterion.
Written by Pendell Meyers A man in his 70s with no cardiac history presented with acute weakness, syncope, and fever. He denied chestpain or shortness of breath. In the clinical context of weakness and fever, without chestpain or shortness of breath, the likelihood of Brugada pattern is obviously much higher.
An adult patient presented with palpitations, chestpain and reduced exertional capacity for 3 years. There was no family history of cardiovascular disease or suddencardiacdeath. Previously, the patient was an amateur weightlifter who used anabolic steroids but had ceased supplements 3 years before admission.
It causes the heart muscle to become stiff and thick, making it harder for the heart to pump blood properly and increasing the risk of suddencardiacdeath. HCM is the most common genetic heart disease worldwide and is estimated to affect 1 in 500 people.
Background On the one hand, the primary coronary slow flow phenomenon (CSFP) can cause recurrence of chestpain, prompting medical examinations and further healthcare costs, while on the other hand, it can lead to myocardial infarction, ventricular arrhythmia and suddencardiacdeath.
He has never had any chestpain. It is crucial for every medical physician to recognize patients who are at risk of suddencardiacdeath due to their underlying medical condition. He has no known prior medical history and does not take any medications. He takes occasional multivitamins.
There was no chestpain. The granulomatous inflammation affects the heart, causing an infiltrative cardiomyopathy The most common manifestations of cardiac sarcoidosis are atrioventricular (AV) block and ventricular tachyarrhythmias (VT). This was written by Magnus Nossen The patient is a female in her 50s.
New HCM Guidelines Updated recommendations in the guideline reflect recent evidence about HCM treatment and management including new forms of pharmacologic management; participation in vigorous recreational activities and competitive sports; and risk stratification for suddencardiacdeath (SCD) with an emphasis on pediatric patients.
Transcript of the video: Brugada Syndrome was described by Brugada brothers in 1992 as right bundle branch block pattern in anterior leads with ST segment elevation and syncope or suddencardiacdeath and it was later in 1998, that the genetic basis of the disease was identified, with mutations in sodium channel.
There was some dyspnea but no chestpain. HCM is estimated to occur in ~1 in 500 young adults , making it among the most common inherited cardiac disorders. A young man presented with continuous prolonged generalized weakness, lightheadedness, and presyncope. Here is his ECG. This shows LVH, with high voltage.
It was from a patient with chestpain: Note the obvious Brugada pattern. 2017 AHA/ACC/HRS guideline for management of patients with ventricular arrhythmias and the prevention of suddencardiacdeath. The elevated troponin was attributed to either type 2 MI or to non-MI acute myocardial injury.
the optimum QT correction formula for patients with chestpain was found to be unique for each individual ; it is a correction factor that can be calculated real-time for each patient by taking multiple measurements over a range of heart rates. Other Research: According to this study b y Batchvarov et al. ,
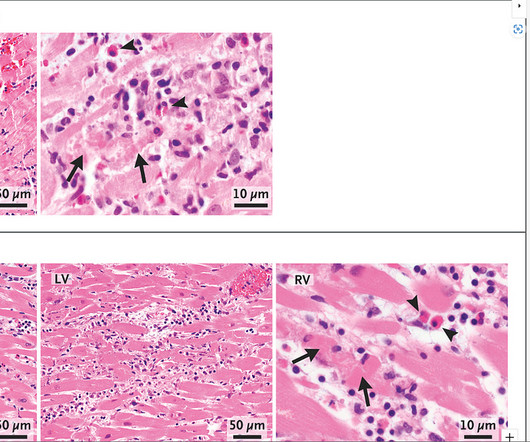
While there are case reports of severe fulminant heart failure and death, the overwhelming majority of patients appear to be able to go home a few days after presentation. The pathological findings are visually fairly obvious - pink healthy cardiac tissue with islands of darkly staining immune cells associated with cell necrosis (death).
Patient 2 : 55 year old with 5 hours of chestpain radiating to the shoulder, with nausea and shortness of breath ECG: sinus bradycardia, normal conduction, normal axis, normal R wave progression, no hypertrophy. This was missed by the treating physician, but the chestpain resolved with aspirin.
The patient denied any chestpain whatsoever, and a troponin at zero and 2 hours were both undetectable. A bedside cardiac ultrasound revealed grossly normal to hyperdynamic systolic function with no obvious areas of wall motion abnormalities. Types 2 and 3 have been merged into Type 2 and look substantially different.
A 50-something male presented to triage with chestpain for one day. A Chest X-ray showed infiltrates. Thus, another etiology of chestpain is found, and the fever suggests "fever-induced Brugada." Unexplained cardiac arrest or documented VF/polymorphic VT: +3 3. The temperature was 39.5 Family History 3.a.
He had no chestpain, dyspnea, or any other anginal equivalent, and his vital signs were normal. The cardiologist thought she had stent thrombosis which is possible, but I do not necessarily think is sufficient to explain her complete hemodynamic collapse.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
























Let's personalize your content