This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
This was sent by anonymous The patient is a 55-year-old male who presented to the emergency department after approximately 3 to 4 days of intermittent central boring chestpain initially responsive to nitroglycerin, but is now more constant and not responsive to nitroglycerin. It is unknown when this pain recurred and became constant.
A 56 year old male with PMHx significant for hypertension had chestpain for several hours, then presented to the ED in the middle of the night. He reported chestpain that developed several hours prior to arrival and was 5/10 in intensity. The pain was located in the mid to left chest and developed after riding his bike.
A 50-something male with hypertension and 20- to 40-year smoking history presented with 1 week of stuttering chestpain that is worse with exertion, which takes many minutes to resolve after resting and never occurs at rest. At times the pain does go to his left neck. It is a ssociated with mild dyspnea on exertion.
A 50-something man presented in shock with severe chestpain. Case continued A bedside ultrasound showed diminished LV EF and of course bradycardia. Angiogram: Culprit Lesion (s): Thrombotic occlusion of the proximal RCA -- stented. His prehospital ECG was diagnostic of inferior posterior OMI.
Submitted and written by Anonymous, edits by Meyers and Smith A 50s-year-old patient with no known cardiac history presented at 0045 with three hours of unrelenting central chestpain. The pain was heavy, radiated to her jaw with an associated headache. A single DES stent was placed, and the patient did well post-procedure.
It is of an elderly woman who complained of shortness of breath and had a recent stent placed. What I had not told him before he made that judgement is that the patient also had ultrasound B-lines of pulmonary edema. Also, we know the patient had a stent. Finally, the presentation is dyspnea, not chestpain.
A 63 year old man with a history of hypertension, hyperlipidemia, prediabetes, and a family history of CAD developed chestpain, shortness of breath, and diaphoresis after consuming a large meal at noon. He called EMS, who arrived on scene about two hours after the onset of pain to find him hypertensive at 220 systolic.
Submitted by Benjamin Garbus, MD with edits by Bracey, Meyers, and Smith A man in his early 30s presented to the ED with chestpain described as an “explosion" of left chest pressure. Today’s pain lasted around 20 mins, but was severe enough that the patient called EMS. Triage EKG: What do you think?
A male in his 40's who had been discharged 6 hours prior after stenting of an inferoposterior STEMI had sudden severe SOB at home 2 hours prior to calling 911. He had no chestpain. He had diffuse crackles on exam and B-lines on chestultrasound, and chest x-ray also confirmed pulmonary edema.
A man in his mid 60s with history of CAD and stents experienced sudden onset epigastric abdominal pain radiating up into his chest at home, waking him from sleep. He had active chestpain at the time of triage at 0137 at night, with this triage ECG: What do you think? Gallbladder ultrasound was negative for stones.
ChestPain – Benign Early Repol or OMI? Written by Destiny Folk, MD, Adam Engberg, MD, and Vitaliy Belyshev MD A man in his early 60s with a past medical history of hypertension, type 2 diabetes, obesity, and hyperlipidemia presented to the emergency department for evaluation of chestpain.
He underwent coronary stenting (uncertain which artery). There is no way to tell the difference between GI etiology of chestpain and MI. Such T-waves are almost always reciprocal to ischemia in the region of aVL (although aVL looks n ormal here) , and in a patient with chestpain are nearly diagnostic of ischemia.
He had no previous history of CAD, and presented with very typical waxing and waning chestpain, much worse with exertion but also present at rest and on presentation, though his pain was minimal at the time of the ECG. Two stents were placed. I saw this 59 year old male 3 weeks ago. Blood pressure was 150/80.
He had concurrent sharp substernal chestpain that resolved, but palpitations continued. Over past 3 months, he has had similar intermittent episodes of sharp chestpain while running, but none at rest. Past medical history includes coronary stenting 17 years prior. However, this is not SVT. What to do now?
Jesse McLaren (@ECGcases), of Emergency Medicine Cases Reviewed by Pendell Meyers and Steve Smith An 85yo with a history of hypertension developed chestpain and collapsed, and had bystander CPR. On arrival, GCS was 13 and the patient complained of ongoing chestpain. So the RCA was stented.
Description of Case:A 64-year-old male with complex medical history, including infective endocarditis of the aortic valve requiring surgical replacement with a bioprosthetic valve and recurrent infective endocarditis of the bioprosthetic valve, presented with two hours of crushing chestpain and found to have ST elevations.
The patient said his chestpain was 4/10, down from 8/10 on presentation. On intravascular ultrasound (IVUS), the mid RCA plaque was described as "cratered, inflamed, and bulky," and the OM plaque was described as "bulky with evidence of inflammation and probably ulceration." Repeat hsTnI was 183 ng/L, up from 26 ng/L.
Written by Willy Frick A 40 year old woman was at home cooking when she developed chestpain. Fortunately, this operator used intravascular ultrasound (IVUS). The operator documented thoughtful consideration of risks and benefits of stent placement. She took an oxycodone and called EMS. I sent this to Drs.
A 60-something man presented by EMS with 5 hours of fairly typical sounding substernal chestpain. EMS gave 324 mg aspirin and 3 sublingual NTG, which the patient stated reduced the substernal chestpain from an 8/10 to 4/10. This was a point of care ultrasound, not a bubble contrast echo.
This is the EKG of a previously healthy 40 year old man with one hour of chestpain and profound weakness and sense of "doom". A bedside ultrasound revealed a possible anterior wall motion abnormality. There was an LAD occlusion that was opened and stented. Click here for an even better case of this phenomenon.
This is the initial ED ECG of a 46 year old male with chestpain: The QTc was 420 ST Elevation at 60 ms after the J-point in lead V3 = 2.5 ng/ml) A 45 year old male called 911 for chestpain: The QTc was 400 ST Elevation at 60 ms after the J-point in lead V3 = 3.5 100% LAD occlusion. He underwent CABG. QRS V2 = 15.5
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chestpain. He described it as "10/10" intensity, radiating across his chest from right to left. This is written by Willy Frick, an amazing cardiology fellow in St.
A middle-aged male with h/o CAD and stents presented with typical chest pressure. Case 3 : Male in 30's with chestpain, cough, and fever. A bedside ultrasound was done by the emergency physician, using Speckle Tracking. A male in late middle age with a history of RCA stent 8 years prior complained of chestpain.
No chestpain. His ED cardiac ultrasound (which is not at all ideal for detecting wall motion abnormalities, and is also very operator dependent for this finding) was significant for depressed global EF. Later on during the night of his admission he had a short episode of chestpain that resolved with sublingual nitroglycerin.
Case A 47 year old male called 911 for severe chestpain. It was opened and stented. A woman in her 60s with no prior history of CAD presented with 3 hours of sharp, centrally located chestpain with radiation to the anterior neck, with associated nausea. Culprit, stented) 3. He was clammy and looked unwell.
To, me these look like anterior wall motion abnormality, but I showed them to one of our ultrasound fellows who is very interested in this. It was stented. Serial ECGs correlated to the presence ( and severity ) of chestpain — often reveal the status of the "culprit" artery (ie, occluded, reopened, reoccluded ).
This was diagnosed by IVUS (intravascular ultrasound) as a ruptured plaque. It was stented. Values: STE60V3 = 2.0, QRS V2 = 10, RAV4 = 15.5, QTc = 377 by computer 4-variable formula value = 16.2, There was good flow. A 0-hour troponin I, drawn 2 hours after symptoms onset , was below the level of detection (LoD, less than 0.010 ng/mL.
A late middle-aged man presented with one hour of chestpain. Bedside ultrasound showed no effusion and moderately decreased LV function, with B-lines of pulmonary edema. This was stented. Most recent echo showed EF of 60%. He also had a history of chronic kidney disease, stage III. He had recently had a NonSTEMI.
Written by Willy Frick A 51 year old man with hypertension presented with three hours of acute onset, severe midsternal chestpain associated with two episodes of nausea and vomiting. or 2) Inferior and lateral OMI that is beginning to reperfuse, even though the patient still has chestpain? ECG 1 What do you think?
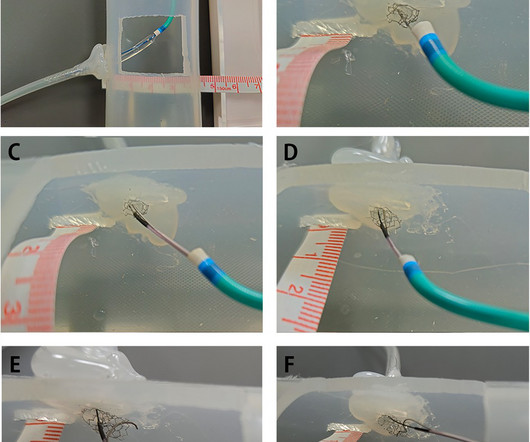
BackgroundPercutaneous coronary intervention (PCI) through the aorto-ostial coronary stent that is protruding into the aorta remains a technical challenge because of the poor coaxial alignment of the guiding catheter and the inability to advance the guidewire into the distal vessel through the stent's central lumen.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




































Let's personalize your content