Post-stent chest pain, revisited
Heart Sisters
JULY 28, 2024
Heart patients with persistent or recurrent post-stent chest pain present “an unmet clinical need”, according to the European Journal of Cardiology.
 Chest Pain Stent Stents
Chest Pain Stent Stents 
Heart Sisters
JULY 28, 2024
Heart patients with persistent or recurrent post-stent chest pain present “an unmet clinical need”, according to the European Journal of Cardiology.
Frontiers in Cardiovascular Medicine
MARCH 16, 2025
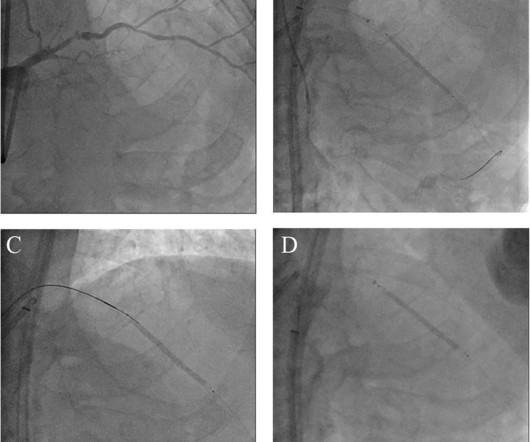
BackgroundAn undeflatable stent balloon following its inflation during percutaneous coronary intervention (PCI) is a rare and unpredictable complication that can lead to serious consequences. Currently, there is no standardized protocol for managing this issue.Case presentationAn 83-year-old man presented with chest pain.

Dr. Smith's ECG Blog
MAY 29, 2024
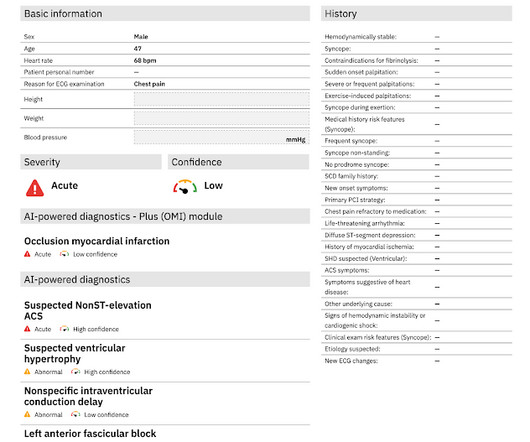
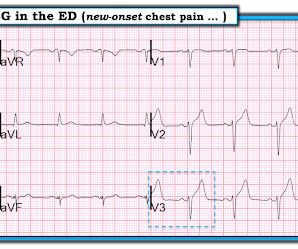
Written by Pendell Meyers Two patients with acute chest pain. Patient 1: Patient 2: Patient 1: A man in his 40s with minimal medical history presented with acute chest pain radiating to his R shoulder. Two patients with chest pain. Do either, neither, or both have OMI and need reperfusion?

Dr. Smith's ECG Blog
MARCH 19, 2024
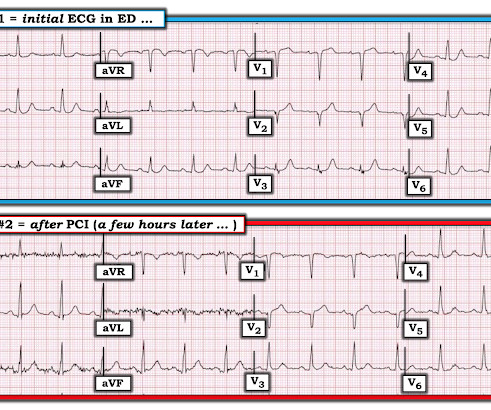
The patient presented to an outside hospital An 80yo female per triage “patient presents with chest pain, also hurts to breathe” PMH: CAD, s/p stent placement, CHF, atrial fibrillation, pacemaker (placed 1 month earlier), LBBB. HPI: Abrupt onset of substernal chest pain associated with nausea/vomiting 30 min PTA.
Medical Xpress - Cardiology
NOVEMBER 7, 2024
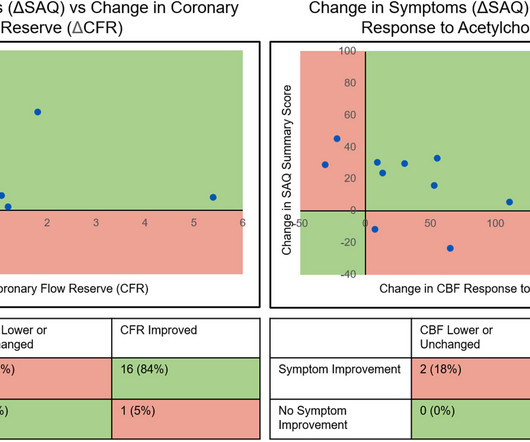
A study at Mayo Clinic suggests that an hourglass-shaped stent could improve blood flow and ease severe and reoccurring chest pain in people with microvascular disease. Of 30 participants in a phase 2 clinical trial, 76% saw improvement in their day-to-day life.

Dr. Smith's ECG Blog
MARCH 31, 2024
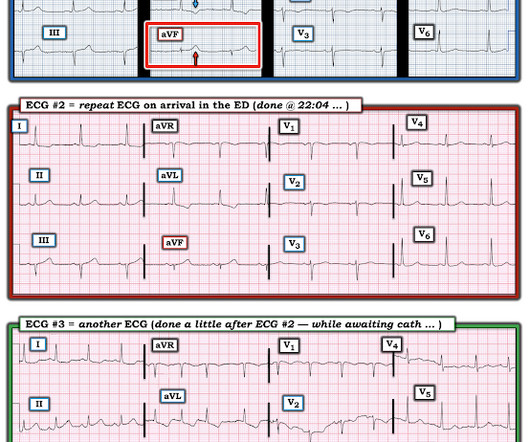
The patient was a middle-aged female who had acute chest pain of approximately 6 hours duration. The pain was still active at the time of evaluation. Angiogram reportedly showed acute thrombotic occlusion of the first obtuse marginal which was stented. Peak troponin was not recorded. Long term follow up is unavailable.

Dr. Smith's ECG Blog
SEPTEMBER 11, 2024
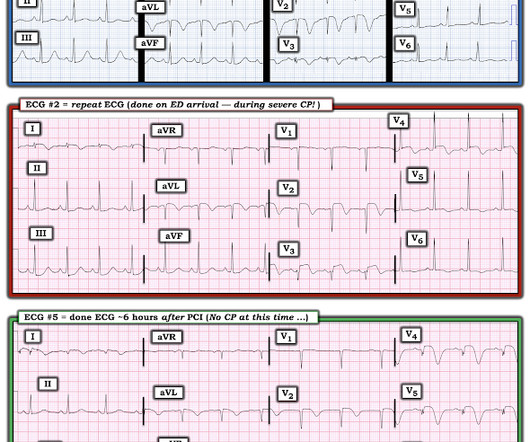
No Chest Pain, but somnolent. The fact that this is syncope makes give it a far lower pretest probability than chest pain, but it was really more than syncope, as the patient actually underwent CPR and had hypotension on arrival of EMS. Former resident: "Just saw cath report, LAD stent was 100% acutely occluded."

Expert insights. Personalized for you.

































Let's personalize your content