This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A 50-something male with hypertension and 20- to 40-year smoking history presented with 1 week of stuttering chestpain that is worse with exertion, which takes many minutes to resolve after resting and never occurs at rest. At times the pain does go to his left neck. It is a ssociated with mild dyspnea on exertion.
He was given aspirin and sublingual nitro and the pain resolved. Bedside cardiac ultrasound with no obvious wall motion abnormalities. Another ECG was recorded after the nitroglycerine and now without pain: All findings are resolved. He had a previous ECG on file: Proving the findings are new The cath lab was activated.
A 63 year old man with a history of hypertension, hyperlipidemia, prediabetes, and a family history of CAD developed chestpain, shortness of breath, and diaphoresis after consuming a large meal at noon. He called EMS, who arrived on scene about two hours after the onset of pain to find him hypertensive at 220 systolic.
Submitted and written by Megan Lieb, DO with edits by Bracey, Smith, Meyers, and Grauer A 50-ish year old man with ICD presented to the emergency department with substernal chestpain for 3 hours prior to arrival. At this time he reported ongoing chestpain and was given aspirin and nitroglycerin. J Am Heart Assoc.
There was no chestpain or SOB at the tim of the ECG: Computerized QTc is 464 ms A previous ECG from 8 years prior was normal. My opinion was that it was not a cath lab case, but I did suggest they do a bedside ultrasound to look for an anterior wall motion abnormality. I had not seen the cardiac ultrasounds at this time.
A 70-something female with no previous cardiac history presented with acute chestpain. She awoke from sleep last night around 4:45 AM (3 hours prior to arrival) with pain that originated in her mid back. She stated the pain was achy/crampy. Over the course of the next hour, this pain turned into a pressure in her chest.
This case was provided by Spencer Schwartz, an outstanding paramedic at Hennepin EMS who is on Hennepin EMS's specialized "P3" team, a team that receives extra training in advanced procedures such as RSI, thoracostomy, vasopressors, and prehospital ultrasound. On medic arrival, she walked out of the house in no distress, but was diaphoretic.
If you saw this ECG only knowing that it is an acute chestpain patient, what would be your interpretation? However, in the context of the first ECG and the waning chestpain, this is diagnostic of reperfusion. Due to the severity of the pain and the high BP, they obtained an aortic dissection CT.
3 hours prior to calling 911 he developed typical chestpain. 1.196 x STE60 in V3 in mm) + (0.059 x computerized QTc) - (0.326 x RA in V4 in mm) Third, one can do an immediate cardiac ultrasound. Medics gave him nitroglycerine sublingual and his pain resolved. The patient had a critical LAD stenosis.
24: Joint American College of Cardiology/Journal of the American College of Cardiology Late-Breaking Clinical Trials (Session 402) Saturday, April 6 9:30 – 10:30 a.m.
Written by Pendell Meyers A man in his late 40s with several ACS risk factors presented with a chief complaint of chestpain. Several hours prior to presentation, while driving his truck, he started experiencing new central chestpain, without radiation, aggravating/alleviating factors, or other associated symptoms.
A middle aged man had off and on chestpain for 2 weeks, then 2 hours of more severe and constant pain. Angiogram Left main: Severe calcific stenosis of ostial and distal left main. LAD: large caliber vessel with severe calcific stenosis of the proximal LAD with TIMI2 flow. He did not get prehospital activation.
This is the initial ED ECG of a 46 year old male with chestpain: The QTc was 420 ST Elevation at 60 ms after the J-point in lead V3 = 2.5 ng/ml) A 45 year old male called 911 for chestpain: The QTc was 400 ST Elevation at 60 ms after the J-point in lead V3 = 3.5 Angiogram showed a critical LAD thrombotic stenosis.
Case A 47 year old male called 911 for severe chestpain. A woman in her 60s with no prior history of CAD presented with 3 hours of sharp, centrally located chestpain with radiation to the anterior neck, with associated nausea. LM: No significant stenosis. D3 has a 95% tubular ostial stenosis.
It was edited by Smith CASE : A 52-year-old male with a past medical history of hypertension and COPD summoned EMS with complaints of chestpain, weakness and nausea. Smith comment: This patient did not have a bedside ultrasound. The paramedic’s initial impression of the patient was that he was critically ill.
Written by Willy Frick A 40 year old woman was at home cooking when she developed chestpain. The cardiologist called this 20% stenosis. Fortunately, this operator used intravascular ultrasound (IVUS). Unfortunately, a few hours later the patient complained of recurrent chestpain. I sent this to Drs.
The patient said his chestpain was 4/10, down from 8/10 on presentation. The LAD has diffuse disease with a few areas of moderate stenosis but no flow-limiting lesions. Remember that patients with OMI can have normal ECGs! Repeat hsTnI was 183 ng/L, up from 26 ng/L. Around noon, cardiology was called for evaluation.
The best course is to wait until the anatomy is defined by angio, then if proceeding to PCI, add Cangrelor (an IV P2Y12 inhibitor) I sent the ECG and clinical information of a 90-year old with chestpain to Dr. McLaren. 2 cases of Aortic Stenosis: Diffuse Subendocardial Ischemia on the ECG. Anything more on history? Left main?
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chestpain. He described it as "10/10" intensity, radiating across his chest from right to left. Fortunately, that is exactly what happened.
Case Continued Bedside ultrasound was performed: This shows an anterior wall motion abnormality, and highly suggests the LAD as the infarct artery. FYI : 52 ng/L is the threshold for "rule in" by European studies as it has a high positive predictive value in the setting of chestpain.
There was no chestpain. So we did a bedside cardiac ultrasound. Acute posterior OMI would be a prime concern for the ECG in Figure-1 — IF the patient presented with cardiac-sounding chestpain. But today's patient had no chestpain. That condition is tricuspid stenosis, which is rare.
To, me these look like anterior wall motion abnormality, but I showed them to one of our ultrasound fellows who is very interested in this. She was treated medically for NonSTEMI, pending next day cath, which showed ulcerated plaque and a 60% thrombotic stenosis in the LAD distal to the first diagonal. She said: This is a tough one.
They had difficulty describing their symptoms, but complained of severe weakness, nausea, vomiting, headache, and chestpain. They described the chestpain as severe, crushing, and non-radiating. Altogether, this strongly suggests inferolateral OMI, particularly in a patient with acute chestpain.
ChestPain – Benign Early Repol or OMI? Written by Destiny Folk, MD, Adam Engberg, MD, and Vitaliy Belyshev MD A man in his early 60s with a past medical history of hypertension, type 2 diabetes, obesity, and hyperlipidemia presented to the emergency department for evaluation of chestpain.
Most cases go undiagnosed until the condition advances enough to create symptoms such as shortness of breath, chestpain or fatigue. AI algorithms could further improve care by using data from ultrasounds and other imaging devices to develop a digital twin of each patient.
The patient in today’s case is a previously healthy 40-something male who contacted EMS due to acute onset crushing chestpain. The pain was 10/10 in intensity radiating bilaterally to the shoulders and also to the left arm and neck. Angiography : LMCA — 90-99% osteal stenosis. The below ECG was recorded.
Case 3 : Male in 30's with chestpain, cough, and fever. A bedside ultrasound was done by the emergency physician, using Speckle Tracking. Is there likely to be fixed coronary stenosis that led to demand ischemia during pneumonia? --Was What do you think? He has clinical pneumonia. Called 911.
Aortic Dissection, Valvular (especially Aortic Stenosis), Tamponade. Check : [vitals, SOB, ChestPain, Ultrasound] If the patient has Abdominal Pain, ChestPain, Dyspnea or Hypoxemia, Headache, Hypotension , then these should be considered the primary chief complaint (not syncope).
A 69 year old woman with a history of hypertension presented to the emergency department by EMS for evaluation of chestpain and shortness of breath. She awoke in the morning with sharp chestpain which worsened throughout the morning. As her pain worsened, so did her dyspnea. This was written by Hans Helseth.
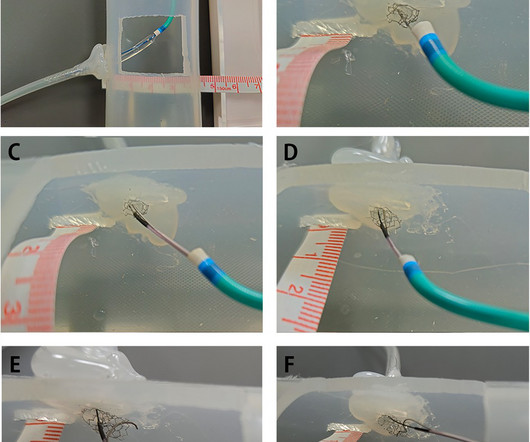
In this article, we introduce a dual-lumen microcatheterfacilitated wiring technique performed on two patients to overcome this difficulty.Case summaryThe first case was a 75-year-old man who presented with chestpain. Despite several attempts, the guidewire passed through the side strut of the stent instead of the central stent lumen.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



































Let's personalize your content