This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A 50-something male with hypertension and 20- to 40-year smoking history presented with 1 week of stuttering chestpain that is worse with exertion, which takes many minutes to resolve after resting and never occurs at rest. At times the pain does go to his left neck. What do you think the prehospital ECG showed (with pain)?
Sent by Drew Williams, written by Pendell Meyers A man in his 50s with history of hypertension was standing at the bus stop when he developed sudden onset severe pressure-like chestpain radiating to his neck and right arm, associated with dyspnea, diaphoresis, and presyncope. When is it anterior STEMI? Is this Acute Ischemia?
A 70-year-old man calls 911 after experiencing sudden, severe chestpain. The precordial ST-depression pattern on this ECG (and in this clinical setting) should immediately raise suspicion of Posterior STEMI! But if there is none - then you are looking at least at an Isolated Posterior STEMI until proven otherwise.
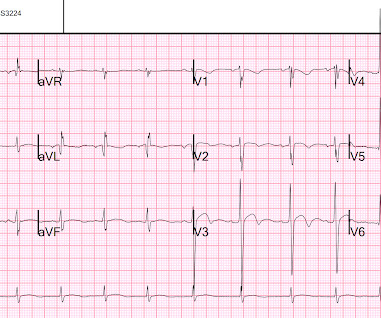
There is clearly sufficient STE for STEMI criteria in leads V2 and aVL, but lead I has less than 1.0 mm of STE - thus, technically this ECG does not meet STEMI criteria, although it is a quite obvious OMI. This ECG was immediatel y discussed with the on-call cardiologist who said the ECG was "concerning but not a STEMI."
He had suffered a couple bouts of typical chestpain in the last 24 hours. This ECG (ECG #3) was recorded immediately after the last episode of pain spontaneously resolved. The pain had lasted about one hour. So you are going to get to see what the ECG would have shown had you recorded one during pain! Am Heart J.
He reports significant chestpain at the base of his scapula on the right side along with new shortness of breath. Smith : there is some minimal ST elevation in V2-V6, but does not meet STEMI criteria. Transient STEMI has been studied and many of these patients will re-occlude in the middle of the night. Is it normal STE?
This was my thought: if this patient presented to the ED with chestpain, then this is an LAD occlusion. His ECG was repeated at this point: This shows a well developed anterior STEMI. To not see these findings is very common, and this patient would be given the diagnosis of NonSTEMI, with subsequent development of STEMI.
This male in his 40's had been having intermittent chestpain for one week. He awoke from sleep with crushing central chestpain and called ems. EMS recorded a 12-lead, then gave 2 sublingual nitros with complete relief of pain. Type B waves are deeper and symmetric. Am J Cardiol (1995) 75 : pp 1206-1210.
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. aVR ST segment elevation: acute STEMI or not? His response: “subendocardial ischemia.
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chestpain. He described it as "10/10" intensity, radiating across his chest from right to left. This is written by Willy Frick, an amazing cardiology fellow in St.
Time window s for intervention for thrombolysis in STEMI starts from onset of chestpain, but when it comes to primary PCI, a different time window takes the center stage pushing the former to the background. How can we have uniform std of 90-120 minutes D2B in all STEMI cases ? Why is this disparity?
A middle-aged woman had intermittent angina for 48 hours, then onset of constant, crushing chestpain for 1.5 cm diameter in the apex The presence of thrombus led the clinicians to state that this was a "late presentation STEMI." hours when she called 911. LV Thrombus , 1.5 0 0 1 95 544 MMRF 4 1 638 14.0 Methods: Vermeer et al.
Case An elderly patient had acute chestpain and 911 was called. Blinded physicians adjudicated angiogram reports for coronary lesions and thrombolysis in myocardial infarction (TIMI) flow score. It is important for cardiologists to realize that a paramedic may see something they do not. What do you think?
He has a history of coronary artery disease and a STEMI two years prior that was treated with primary PCI. He contacted EMS due to acute onset chestpain and feeling unwell and fatigued. He subsequently developed worsening chestpain. Pain is improving and ischemic T-wave inversions are no longer present".
The ECG in Figure-1 was obtained from a middle-aged man who presents to the ED ( E mergency D epartment ) with 6 hours of chestpain. Figure-1: The initial ECG in today's case obtained from a middle-aged man with 6 hours of chestpain. ( He is hemodynamically stable.
A middle-age woman with no previous cardiac history called 911 for chestpain. The paramedics diagnosis was "Possible Anterolateral STEMI." More proof that a huge STEMI may have normal or near normal initial troponin. Taken together, these findings suggest an ongoing extensive antero-lateral STEMI.
A 30 year old African American Male presented to the ED with chestpain that occurred the day before. There was no pain on the day of presentation. 2019.06.007) (Full text here: [link] ) The ECG above is diagnostic of Wellens' syndrome (full reference below): 1) Episode of anginal chestpain that is resolved (GONE!)
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.























Let's personalize your content