This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Written by Pendell Meyers Two patients with acute chestpain. Patient 1: Patient 2: Patient 1: A man in his 40s with minimal medical history presented with acute chestpain radiating to his R shoulder. Two patients with chestpain. Do either, neither, or both have OMI and need reperfusion?
The patient was a middle-aged female who had acute chestpain of approximately 6 hours duration. The pain was still active at the time of evaluation. The interventional cardiologist then canceled the activation and returned the patient to the ED without doing an angiogram ("Not a STEMI"). mm STE in the posterior leads.
Written by Jesse McLaren A healthy 75 year old developed 7/10 chestpain associated with diaphoresis and nausea, which began on exertion but persisted. Below is the first ECG recorded by paramedics after 2 hours of chestpain, interpreted by the machine as “possible inferior ischemia”. What do you think?
The patient presented to an outside hospital An 80yo female per triage “patient presents with chestpain, also hurts to breathe” PMH: CAD, s/p stent placement, CHF, atrial fibrillation, pacemaker (placed 1 month earlier), LBBB. HPI: Abrupt onset of substernal chestpain associated with nausea/vomiting 30 min PTA.
Written by Jesse McLaren, comments by Smith A 55 year old with a history of NSTEMI presented with two hours of exertional chestpain, with normal vitals. Old ‘NSTEMI’ A history of coronary artery disease and a stent to the same territory further increases pre-test likelihood of acute coronary occlusion, including in-stent thrombosis.
A 50-something male with hypertension and 20- to 40-year smoking history presented with 1 week of stuttering chestpain that is worse with exertion, which takes many minutes to resolve after resting and never occurs at rest. At times the pain does go to his left neck. What do you think the prehospital ECG showed (with pain)?
A 60 yo with 2 previous inferior (RCA) STEMIs, stented, called 911 for one hour of chestpain. Here is his most recent previous ECG: This was recorded after intervention for inferior STEMI (with massive ST Elevation, see below), and shows inferior Q-waves with T-wave inversion typical of completed inferior OMI.
Written by Willy Frick A man in his 50s with history of hypertension, hyperlipidemia, and a 30 pack-year smoking history presented to the ER with 1 hour of acute onset, severe chestpain and diaphoresis. For national registry purposes, this will be incorrectly classified as a STEMI.) Most STEMI have peak cTnI greater than 10.0.
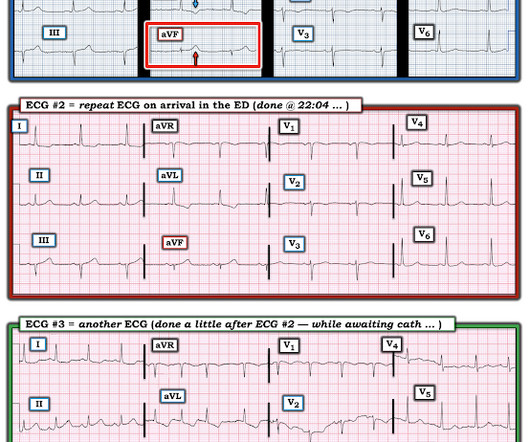
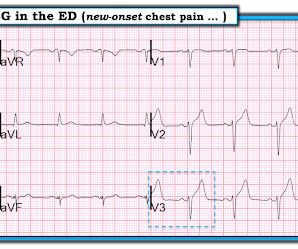
Written by Magnus Nossen with Edits by Grauer and Smith The ECGs in today’s case are from 3 different patients all presenting with new-onset CP ( ChestPain ). It definitely does not fulfill STEMI criteria, and I would argue that it would not lead to cath lab activation in most centers. The ECG shows ST depression in lead V3.
Theres ST elevation in V3-4 which meets STEMI criteria, which could be present in either early repolarization, pericarditis or injury. Lets see what happens in the current STEMI paradigm. Emergency physician: STEMI neg but with elevated troponin = Non-STEMI The first ECG was signed off. Chestpain still persists.
I was working at triage when the medics brought this patient who is 65 yo and has had chestpain for 12 hours. Another ECG was recorded while awaiting the cath team: Now there is STEMI Let's look at that first (prehospital ECG) again: Very subtle! It was opened and stented. So I uncrumpled it: What do you think?
Written by Pendell Meyers A man in his early 40s experienced acute onset chestpain. The chestpain started about 24 hours ago, but there was no detailed information available about whether his pain had come and gone, or what prompted him to be evaluated 24 hours after onset. And yet it still says "normal".
A 40-something male presented by ambulance with one hour of chestpain that was improving after sublingual nitroglycerine and 325 mg of aspirin, chewed. Here it is: Obvious Inferior Posterior STEMI (+) OMI. Initial troponin was: 3 ng/L We showed that the first troponin in acute STEMI is often negative in at least 27%.
Written by Jesse McLaren A previously healthy 50 year-old presented with 24 hours of intermittent exertional chestpain, radiating to the arms and associated with shortness of breath. In a previously healthy patient with new and ongoing chestpain, this is concerning for acute occlusion of the first diagonal artery.
A male in his 40's who had been discharged 6 hours prior after stenting of an inferoposterior STEMI had sudden severe SOB at home 2 hours prior to calling 911. He had no chestpain. Is this acute STEMI? Is this an acute STEMI? -- Unlikely! Medications were aspirin, clopidogrel, metoprolol, and simvastatin.
A 50-something man presented in shock with severe chestpain. There is an obvious inferior posterior STEMI(+) OMI. Angiogram: Culprit Lesion (s): Thrombotic occlusion of the proximal RCA -- stented. Results Of 149 patients with inferior STEMI , 43 (29%) had RVMI and 106 (71%) did not. What is the atrial activity?
Written by Jesse McLaren A 70 year old with prior MIs and stents to LAD and RCA presented to the emergency department with 2 weeks of increasing exertional chestpain radiating to the left arm, associated with nausea. of such ‘high risk Non-STEMI’ patients get angiography within 2 hours.[2] But does this matter?
52-year-old lady presents to the Emergency Department with 2 hours of chestpain, palpitations & SOB. These elevations meet STEMI criteria ( ≥ 1mm in 2 contiguous leads). In STEMI, they are generally upright and large in proportion to the QRS. So this argues against acute STEMI.
This is another case written by Pendell Meyers (who is helping to edit the blog and has many great recent posts) Case A 45 year old man was driving to work when he experienced acute onset sharp left sided chestpain with paresthesias of the left arm. A repeat ECG was recorded with pain 2/10: Not much change.
male was sitting at a work conference when he began having substernal chestpain with diaphoresis. The pain was 7 out of 10 when this ECG was recorded: The QTc = 375 What do you think? Since the threshold for "STEMI" is 2.0 mm, this ECG actually meets STEMI criteria. Since the threshold for "STEMI" is 2.0
A 63 year old man with a history of hypertension, hyperlipidemia, prediabetes, and a family history of CAD developed chestpain, shortness of breath, and diaphoresis after consuming a large meal at noon. He called EMS, who arrived on scene about two hours after the onset of pain to find him hypertensive at 220 systolic.
Sent by anonymous, written by Pendell Meyers A man in his 60s presented with acute chestpain with diaphoresis. Diagnosis: Acute non-ST segment elevation MI (Non-STEMI, or NSTEMI) Second troponin returned at around 0200: 15,894 ng/L 0245 (unclear if ongoing pain or not) Inferoposterior (and lateral V5-6) reperfusion findings.
A middle aged male presented at midnight after 14 hours of constant, severe substernal chestpain, radiating to his throat and to bilateral jaws, and associated with diaphoresis. The pain was not positional, pleuritic, or reproducible. The "criteria" for posterior STEMI are 0.5 Is it STEMI or NonSTEMI?
Submitted and written by Anonymous, edits by Meyers and Smith A 50s-year-old patient with no known cardiac history presented at 0045 with three hours of unrelenting central chestpain. The pain was heavy, radiated to her jaw with an associated headache. A single DES stent was placed, and the patient did well post-procedure.
These tall T waves are associated with flattening ( straightening ) of the ST segment in the inferior leads — with slight S T elevation in leads V2-thru-V6 ( albeit not enough to qualify as a "STEMI" — Akbar et al, StatPearls, 2023 ). Figure-2: Comparison between the 2 ECGs recorded in today's case.
Written by Pendell Meyers, with edits by Steve Smith A man in his early 40s with history of MI s/p PCI presented with bilateral anterior chestpain described as burning and belching with no radiation since last night starting around 11pm (roughly 11 hours ago). But it does not meet STEMI criteria and it was not initially recognized.
Chris Mondie of the Newark Beth Israel Emergency Medicine Residency sent this case A 50-something man presented with acute chestpain. So there is definitely no STEMI, and the STE is normal. But after reading this blog, you all know that most OMI do NOT meet STEMI criteria. 100% proximal LAD successfully stented.
A 60-something woman called EMS for chestpain. link] Clinical Course I don't know if the medics noticed these ECG findings or not, but if not, they recognized the value of serial ECGs in a patient with chestpain. The medics administered aspirin (no Nitroglycerine), and the pain resolved. #5: mm in V2 and 0.65
Written and submitted by Ashley Mogul, with edits by Pendell Meyers and Steve Smith A man in his 40s with recent smoking cessation but otherwise no known past medical history presented due to chestpain since the previous evening. The pain has been constant and associated with vomiting and diaphoresis.
Sent by Anonymous, written by Pendell Meyers A man in his 60s with history of CAD and 2 prior stents presented to the ED complaining of acute heavy substernal chestpain that began while eating breakfast about an hour ago, and had been persistent since then, despite EMS administering aspirin and nitroglycerin. Pre-intervention.
A 60-something awoke with 10/10 crushing chestpain. I would expect that a stent would be placed. The angiogram showed an open artery with 95% stenosis and thrombosis and it was stented. Quiz : What percent of full blown STEMI have an open artery with normal flow at angiogram? He walked in to triage.
Sent by anonymous A man in his 40s with no previous heart disease presented within 30 minutes of onset of acute chestpain that started while exercising. Now it is a full blown STEMI of 3 myocardial territories: inferior, posterior, and lateral But at least it does not call it "Normal." Chestpain and a computer ‘normal’ ECG.
Case submitted by Rachel Plate MD, written by Pendell Meyers A man in his 70s presented with chestpain which had started acutely at rest and has lasted for 2 hours. The pain was still ongoing at arrival. He also noted a bilateral "odd feeling" in his arms. He stated it was similar to prior heart attacks.
Case written and submitted by Ryan Barnicle MD, with edits by Pendell Meyers While vacationing on one of the islands off the northeast coast, a healthy 70ish year old male presented to the island health center for an evaluation of chestpain. The chestpain started about one hour prior to arrival while bike riding.
He had suffered a couple bouts of typical chestpain in the last 24 hours. This ECG (ECG #3) was recorded immediately after the last episode of pain spontaneously resolved. The pain had lasted about one hour. So you are going to get to see what the ECG would have shown had you recorded one during pain!
The 50-something patient with history of coronary stenting and slightly reduced LV ejection fraction. In the setting of prior stenting and reduced left ventricular ejection fraction, would pursue a heart team revascularization approach Syntax score 28.5, Pericarditis would be even more unlikely in someone without chestpain.
== MY Comment by K EN G RAUER, MD ( 9/17/2020 ): == Todays patient is a previously healthy, 60-something year-old woman who presented with chestpain that began at a reception. We are indebted to Dr. Smith for developing Modified Smith-Sgarbossa Criteria for assessing ST-T wave changes in chestpain patients with LBBB.
The patient had continued to have chestpain. There was a 100% proximal LAD occlusion that was opened and stented. Therefore, the provider had appropriately recorded another ECG (but unfortunately unnecessarily delayed by 45 minutes at 0615): Now it is obvious to everyone, not only to an expert. The cath lab was activated.
He had no previous history of CAD, and presented with very typical waxing and waning chestpain, much worse with exertion but also present at rest and on presentation, though his pain was minimal at the time of the ECG. This is all suggestive of posterior STEMI, but not definitely diagnostic. Two stents were placed.
A man in his mid 60s with history of CAD and stents experienced sudden onset epigastric abdominal pain radiating up into his chest at home, waking him from sleep. He had active chestpain at the time of triage at 0137 at night, with this triage ECG: What do you think? Chest x-ray was normal.
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. He arrived to the ED by helicopter at 1507, about three hours after the start of his chestpain while chopping wood around noon. It was stented.
Echo on the day after admission showed EF of 30-35% and antero-apical wall akinesis with an LV thrombus [these frequently form in complete or near complete (no early reperfusion) anterior STEMI because of akinesis/stasis] 2 more days later, this was recorded: ST elevation is still present. An open 90% LAD was stented.
Written by Pendell Meyers A male in his early 50s presented with waxing and waning chestpain starting at rest. Over the next few hours, four other general cardiologists "signed off on the initial ECG without recognizing STEMI." They found 100% acute mid-LAD Occlusion MI, stented with excellent angiographic result.
Case 1 A middle aged woman presented with acute chestpain and shortness of breath, unclear time since onset, and likely with episodic symptoms off and on throughout the day. Only very slight STE which does not meet STEMI criteria at this time. Another lesion in the proximal LAD with 80% stenosis was stented as well.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.















































Let's personalize your content