

Healthy 45-year-old with chest pain: early repolarization, pericarditis or injury?
Dr. Smith's ECG Blog
SEPTEMBER 25, 2024
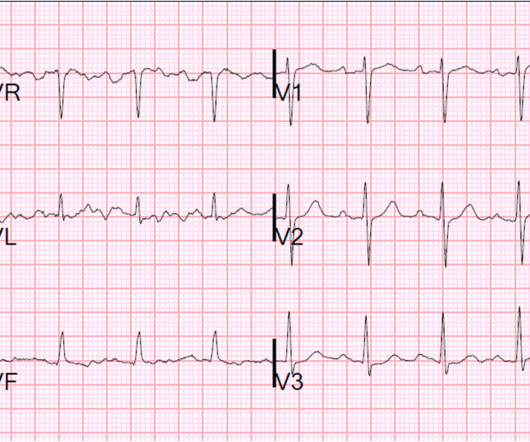
A healthy 45-year-old female presented with chest pain, with normal vitals. The patient was previously healthy, with no atherosclerotic risk factors, and developed chest pain after an episode of stress. The pain was crushing retrosternal, radiated to the arms and was associated with lightheadedness.
































Let's personalize your content