This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Theres ST elevation in V3-4 which meets STEMI criteria, which could be present in either early repolarization, pericarditis or injury. Lets see what happens in the current STEMI paradigm. Emergency physician: STEMI neg but with elevated troponin = Non-STEMI The first ECG was signed off. Chestpain still persists.
A 40-something male presented by ambulance with one hour of chestpain that was improving after sublingual nitroglycerine and 325 mg of aspirin, chewed. Here it is: Obvious Inferior Posterior STEMI (+) OMI. Initial troponin was: 3 ng/L We showed that the first troponin in acute STEMI is often negative in at least 27%.
Sent by anonymous, written by Pendell Meyers A man in his 50s with no prior known medical history presented to the Emergency Department with severe intermittent chestpain. He denied any lightheadedness, shortness of breath, vomiting, or abdominal pain. Barely any STE, and thus not meeting STEMI criteria.
Written by Jesse McLaren, with comments from Smith A 50-year old patient on the medical wards developed acute chestpain, with an ECG labeled (see computer interpretation at the top) and confirmed as normal. In the STEMI paradigm, patients with ischemic symptoms and ECGs that don’t meet STEMI criteria get serial ECGs.
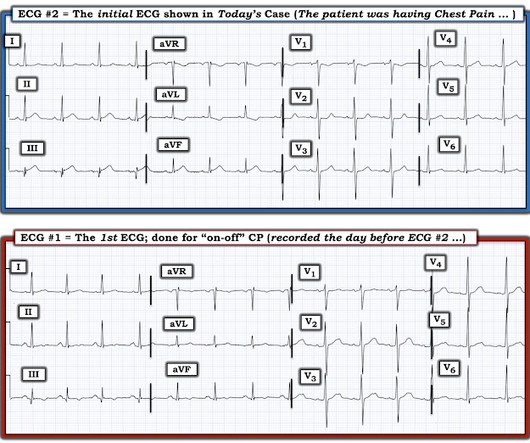
[link] == MY Comment, by K EN G RAUER, MD ( 8/6 /2023 ): == Brilliant talk by Dr. Smith on the state of the art addressing the “need for OMI — and the fallacy of STEMI”. Doing so allows you to put YOURSELF to the TEST ( keeping in mind that all ECGs shown are from patients with chestpain suggestive of potential acute coronary disease ).
He had suffered a couple bouts of typical chestpain in the last 24 hours. This ECG (ECG #3) was recorded immediately after the last episode of pain spontaneously resolved. The pain had lasted about one hour. So you are going to get to see what the ECG would have shown had you recorded one during pain!
Discharge Diagnosis was STEMI (The STE did not meet "criteria," so "OMI" would be better, but "STEMI" is far better than what this could have been called: NonSTEMI) Quotes from a note written by a really fine and knowledgable physician: "12-lead EKG was obtained initial 1 at time zero. Chestpain is squeezing or tight in nature.
He reports significant chestpain at the base of his scapula on the right side along with new shortness of breath. Smith : there is some minimal ST elevation in V2-V6, but does not meet STEMI criteria. Transient STEMI has been studied and many of these patients will re-occlude in the middle of the night. Is it normal STE?
A 40-something male with no previous cardiac disease presented with chestpain. Moreover, the research which appears to confirm this idea was indeed in relation to the circumflex, but they did not study Occlusion ; rather, they studied asymptomatic coronary disease. Here is his ECG: There is no clear evidence of OMI or ischemia.
This is a 58 year old male with 40 minutes of chestpain of acute onset. He called 911 and paramedics recorded a prehospital 12 lead ECG which showed a clear inferior STEMI (not shown, tracing could not be found). He was given aspirin and sublingual nitroglycerine, which improved his pain. This is present here.
A 70-something female with no previous cardiac history presented with acute chestpain. She awoke from sleep last night around 4:45 AM (3 hours prior to arrival) with pain that originated in her mid back. She stated the pain was achy/crampy. Over the course of the next hour, this pain turned into a pressure in her chest.
Furthermore, some ECGs may not meet the STEMI criteria but may still be diagnostic for acute coronary occlusion (ACO). Many researchers, including the editors of this blog, tried to develop such tools in the recent past and we have recommended their use in certain clinical scenarios in many posts on this blog.
This patient, who is a mid 60s female with a history of hypertension, hyperlipidemia and GERD, called 911 because of chestpain. A mid 60s woman with history of hypertension, hyperlipidemia, and GERD called 911 for chestpain. It is also NOT the clinical scenario of takotsubo (a week of intermittent chestpain).
It is equivalent to a transient STEMI. Not much, but studies of STEMI and NonSTEMI show that about 70% of those diagnosed with STEMI have a peak troponin I above 10 ng/mL and that about 70% of those diagnosed with NonSTEMI have a peak troponin I below 10 ng/mL. She has done quite a bit of research on the topic.
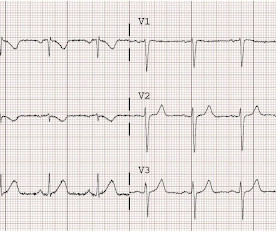
I do research on Cardiologs' algorithm: Smith SW et al. But lead V2 has a worrisome amount of ST elevation, and in a chestpain patient, I would be worried about STEMI. All bets would be off if instead of no chestpain, this patient had worrisome new-onset symptoms. The Ratios of STE to S-wave: V1: 2.5/16
Written by Colin Jenkins and Nhu-Nguyen Le with edits by Willy Frick and by Smith A 46-year-old male presented to the emergency department with 2 days of heavy substernal chestpain and nausea. The patient continued having chestpain. Is there STEMI? Circulation Research , 56 (2), 184–194. link] Fesmire, F.
Written by Jesse McLaren, with comments from Smith An 85 year old with a history of CAD presented with 3 hours of chestpain that feels like heartburn but that radiates to the left arm. There’s minimal concave ST elevation in III which does not meet STEMI criteria, so this ECG is "STEMI negative". Below is the ECG.
Case An elderly patient had acute chestpain and 911 was called. And, in cases like the elderly patient with new-onset chestpain presented here — definitive diagnosis of acute STEMI is sometimes deceptively easy. BOTTOM LINE: Despite cardiac pacing — ECG #2 is diagnostic of a very large acute anterior STEMI.
I remember Allie well from her days in the Research volunteer program at Hennepin. 2) The STE in V1 and V2 has an R'-wave and downsloping ST segments, very atypical for STEMI. Cardiology was consulted and they agreed that the EKG had an atypical morphology for STEMI and did not activate the cath lab. Bicarb 20, Lactate 4.2,
Note: according to the STEMI paradigm these ECGs are easy, but in reality they are difficult. Theres inferior STE which meets STEMI criteria, but this is in the context of tall R waves (18mm) and relatively small T waves, and the STD/TWI in aVL is concordant to the negative QRS. This was false positive STEMI with an ECG mimicking OMI.
Written by Willy Frick A man in his 60s with a history of hypertension and 40 pack-year history presented to the ER with 1 day of intermittent, burning substernal chestpain radiating into both arms as well as his back and jaw. In the world of STEMI, we are incapable of recognizing the first ECG as a false negative.
Dizziness is so unlikely to be OMI without an obvious ECG, that I am going to pretend that this patient presented with chestpain. The PMCardio Queen of Hearts app asks you, before giving an interpretation of OMI ("STEMI-Equivalent"), whether the patient's clinical presentation is high risk for OMI. What do you think?
He had no chestpain, dyspnea, or any other anginal equivalent, and his vital signs were normal. Circulation Research , 114 (12), 18521866. There was indication of parasympathetic overdrive ( the acute inferior STEMI with profound bradycardia and junctional escape ). Journal of Geriatric Cardiology , 19 (6).
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



























Let's personalize your content