This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
In this ECG Cases blog, Jesse McLaren and Rajiv Thavanathan explore how ECG and POCUS complement each other for patients presenting to the emergency department with shortness of breath or chestpain. The post ECG Cases 49 – ECG and POCUS for Dyspnea and ChestPain appeared first on Emergency Medicine Cases.
The increased use of radiofrequency ablation (RFA) for atrial fibrillation (AF) has led to a rise in cases of pulmonary vein stenosis or occlusion (PVS/O) as a complication. The actual frequency of pulmonary vein (PV) occlusion remains a topic of debate.
Written by Pendell Meyers A man in his late 30s with history of hypertension, tobacco use, and obesity presented to the Emergency Department for acute chestpain which started approximately 3 hours prior to arrival, in the setting of a very stressful situation. The pain radiated down both arms, 10/10 in severity. Which is true.
Written by Bobby Nicholson, MD 67 year old male with history of hypertension and hyperlipidemia presented to the Emergency Department via ambulance with midsternal nonradiating chestpain and dyspnea on exertion. Pain improved to 1/10 after EMS administers 324 mg aspirin and the following EKG is obtained at triage.
Written by Jesse McLaren Two patients in their 70s presented to the ED with chestpain and RBBB. Patient 1 : a 75 year old called paramedics with one day of left shoulder pain which migrated to the central chest, which was worse with deep breaths. Ten days later the patient returned with worsening pleuritic chest.
Written by Jesse McLaren, comments by Smith A 55 year old with a history of NSTEMI presented with two hours of exertional chestpain, with normal vitals. See these posts: ChestPain, ST Elevation, and an Elevated Troponin: Should we Activate the Cath Lab? What do you think?
Smith interpretation: This is highly likely to be due to extreme right heart strain and is nearly diagnostic of pulmonary embolism. She had been sitting doing work when she experienced "waves of chest tightness". She had been sitting doing work when she experienced "waves of chest tightness". It is of course pulmonary embolism.
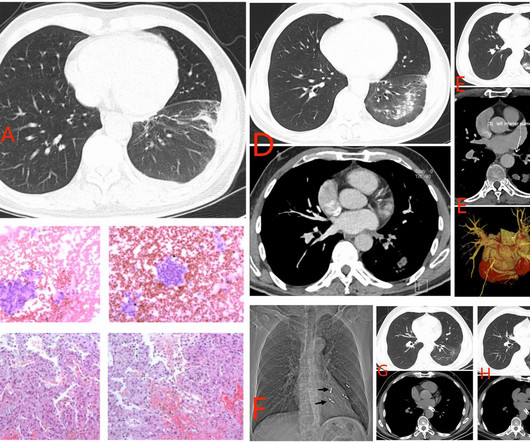
A middle-aged patient with lung cancer had presented to clinic complaining of generalized malaise, cough, and chestpain. Symptoms other than chestpain (malaise, cough in a cancer patient) 2. Inclusion criteria were chestpain, at least 2 serial cTnI in 24 hours, sinus rhythm , and at least 1 ECG.
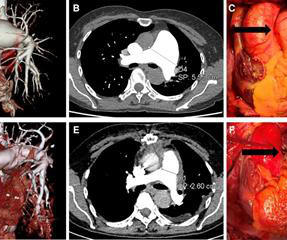
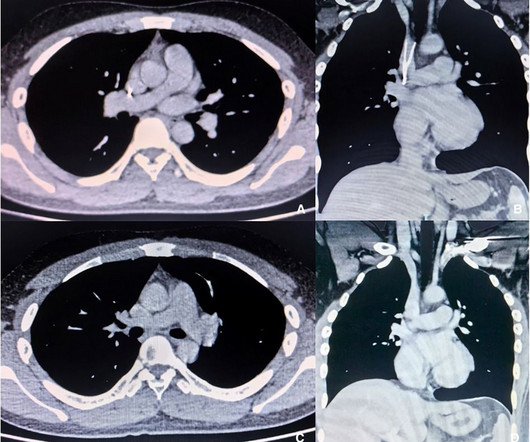
Idiopathic pulmonary aneurysm is a clinically rare condition characterized by an unknown etiology and episodic occurrence. Despite its rarity, idiopathic pulmonary artery aneurysm poses potential risks to patients. Subsequently, she underwent surgical treatment.
The patient's nitro was dialed up to 100 mcg/min but the pain persisted. The ACC/AHA guidelines mandate less than 2 hours cath for patients with ACS with refractory pain, pulmonary edema, or electrical or hemodynamic instability.
In this ECG Cases blog we look at 10 cases of patients with chestpain, including false positive STEMI, false negative STEMI, and other causes to help hone your ECG interpretation skills in time-sensitive cases where those very ECG skills might save a life.
No prior exertional complaints of chestpain, dizziness, lightheadedness, or undue shortness of breath. He denied headache or neck pain associated with exertion. I sent this ECG to Dr. Smith, with the only information that it is a 17 year old with chestpain. 24 yo woman with chestpain: Is this STEMI?
Case written and submitted by Ryan Barnicle MD, with edits by Pendell Meyers While vacationing on one of the islands off the northeast coast, a healthy 70ish year old male presented to the island health center for an evaluation of chestpain. The chestpain started about one hour prior to arrival while bike riding.
A middle aged male presented at midnight after 14 hours of constant, severe substernal chestpain, radiating to his throat and to bilateral jaws, and associated with diaphoresis. The pain was not positional, pleuritic, or reproducible. Patients with ACS and acute pulmonary edema 3. It was not relieved by anything.
This is a previously healthy male teenager who was awoken by chestpain. He was seen at another hospital and found to have a slightly elevated troponin, then underwent a CT pulmonary angiogram (PE) protocol which revealed a right sided pneumonia. In the evening, he became diaphoretic and complained of 9/10 continuous chestpain.
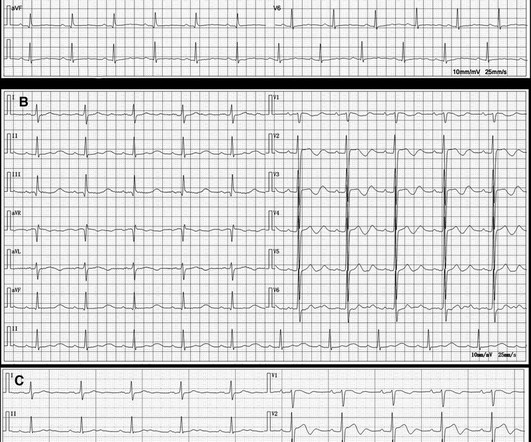
The ECG is rather classic for pulmonary embolism, and indeed this was a large acute PE. More on the ECG in pulmonary embolism: The ECG in this patient has both precordial T-wave inversions AND T-wave inversion in lead III. this is highly suggestive of pulmonary embolism. This is a classic S1Q3T3. Most S1Q3T3 is not due to PE.
We have seen this pattern in many pts with acute right heart strain on this blog. __ Smith : The combination of T-wave inversion in V1-V3 and in lead III is very specific for acute pulmonary embolism. Acute pulmonary embolism was confirmed on CT: The patient did well with treatment. So everything about this ECG screams acute PE.
Submitted by Ali Khan MD and James Mantas MD, MS, written by Pendell Meyers A man in his 50s with history of diabetes, hypertension, and tobacco use presented to the ED with 24 hours of worsening left sided chestpain radiating to the back, characterized as squeezing and pinching, associated with shortness of breath.
Written by Pendell Meyers, with some edits by Smith A man in his 40s with many comorbidities presented to the ED with chestpain, hypotension, dyspnea, and hypoxemia. The bedside echo showed a large RV (Does this mean there is a pulmonary embolism as the etiology?) An 80-something woman who presented with chestpain and dyspnea.
He then went on to say: "40-something with chestpain for one hour. Burning pain subxiphoid and into throat." I’ll emphasize that the generalities stated here may not pertain early on in the process in a patient with a worrisome history of new-onset chestpain. Had episode of nausea and dizziness when it started.
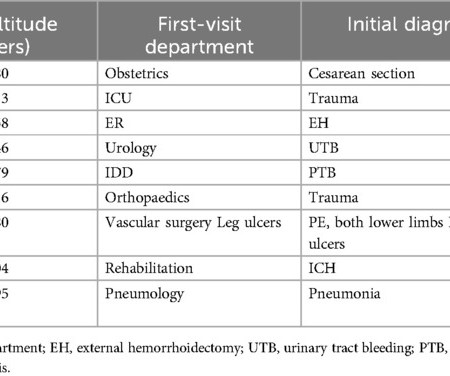
years, and the time from computed tomography pulmonary angiography (CTPA) diagnosis to interventional treatment averaged 2.8 ± 2.2 years, and the time from computed tomography pulmonary angiography (CTPA) diagnosis to interventional treatment averaged 2.8 ± 2.2 m, with an average age of 62.0 ± 16.0 m, with an average age of 62.0 ± 16.0
A 63 year old man with a history of hypertension, hyperlipidemia, prediabetes, and a family history of CAD developed chestpain, shortness of breath, and diaphoresis after consuming a large meal at noon. He called EMS, who arrived on scene about two hours after the onset of pain to find him hypertensive at 220 systolic.
Explanation : The patient had a worrisome history: 59 yo with significant substernal chest pressure, so his pretest probability of MI (and even of STEMI) is reasonably high. Only 5-13% of patients with chestpain and LBBB have MI; many fewer have coronary occlusion. Moreover, and importantly, there was sinus tach.
An 80-something woman who presented with chestpain and dyspnea. An old formal echo was found from 6 mo ago: Dilated right ventricle with septal flattening and estimated right ventricular systolic pressure of 70 mmHg (significant pulmonary hypertension). After all, this patient did also present with chestpain. ) — See below.
He had no chestpain. He was in acute distress from pulmonary edema, with a BP of 180/110, pulse 110. He had diffuse crackles on exam and B-lines on chest ultrasound, and chest x-ray also confirmed pulmonary edema. The hypertension alone is the likely etiology of the pulmonary edema.
A 50-year-old man presented to the emergency department with symptoms of acute chestpain, dizziness, and headache. If the dissection extends into the aortic arch branches, ensuring adequate cerebral perfusion during surgery is crucial to preventing stroke. His blood pressure was 180/110 mmHg and heart rate was 100 bpm.
Genetic protein S (PS) deficiency caused by PROS1 gene mutation is an important risk factor for hereditary thrombophilia.Case introductionIn this case, we report a 28-year-old male patient who developed a severe pulmonary embolism during his visit. The patient had experienced one month of chestpains, coughing and hemoptysis symptoms.
Chronic Pulmonary Disease Lung diseases like chronic obstructive pulmonary disease (COPD) can lead to pulmonary hypertension, which in turn can cause the right side of the heart to enlarge, a condition known as cor pulmonale.
In the evening, a middle-aged man complained of chestpain at the nursing home. His chestpain was vague. He mentioned "cancer" and "chest". Nurses found him with a BP of 50/30 and heart rate of 130 and called EMS. He was awake, with a pulse of 130 and BP of 50/30. Fluids were started.
While in the ED, patient developed acute dyspnea while at rest, initially not associated with chestpain. He later developed mild continuous chestpain, that he describes as the sensation of someone standing on his chest. Xray was consistent with pulmonary vascular congestion. 40 mg of furosemide was given.
Ken (below) is appropriately worried about pulmonary embolism from the ECG. What I had not told him before he made that judgement is that the patient also had ultrasound B-lines of pulmonary edema. Finally, the presentation is dyspnea, not chestpain. What do you think? Also, we know the patient had a stent.
large ASD, partial anomalous pulmonary venous return, significant tricuspid regurgitation, carcinoid valvular disease, etc,) 2) Conditions causing pressure overload of the RV. Any cause of pulmonary hypertension. There is normal axis, normal R-wave progression in the precordial leads and no intraventricular conduction abnormalities.
In patients with narrow QRS ( not this patient), this pattern is highly suggestive of acute pulmonary embolism. Although it was technically difficult and the quality therefore leaves a lot to be desired, you can still make out RV dilation and septal flattening which is much more suggestive of pulmonary embolism than OMI.
He reports significant chestpain at the base of his scapula on the right side along with new shortness of breath. The estimated pulmonary artery systolic pressure is 27 mmHg + RA pressure. Wellen's waves indicate that, when the patient was having chestpain, there was occlusion. A 70-something y.o.
Preoperative ultrasonography and CT examination revealed that the filter retraction hook was very likely to penetrate the SVC wall and its tip was very close to the right pulmonary artery. During this procedure, the patient experienced discomfort, such as chestpain and palpitations, but these symptoms disappeared when procedure completed.
This patient had the onset of chestpain 24 hours before arrival to the ED. I wonder if this patient had pulmonary disease? The relevance of recognizing pulmonary disease on ECG — is that this may sometimes render assessment for acute OMI more difficult — although this was not the case in today's tracing. (
We present a case report of the adverse effects of amiodarone and review its characteristics.Case reportA 73-year-old Asian female with a history of paroxysmal atrial fibrillation managed with amiodarone, well-controlled hypertension, and no substance abuse presented with gastrointestinal distress and dizziness, without chestpain or palpitations.
63 years old Afsar Khan resident of Karwan, Hyderabad had been having coronary artery disease and chestpain on exertion for about a year. With increasing chestpain, he underwent coronary angiography in June. His HRCT chest showed no active Covid 19 lesions and some pulmonary fibrosis.
There was no chestpain or SOB at the tim of the ECG: Computerized QTc is 464 ms A previous ECG from 8 years prior was normal. Absence of chestpain or SOB at the time of the ECG is important; had the patient had active chestpain, I would have recommended at least an emergency formal echo, if not cath lab activation.
56 y/o male who presented with 12/10 severe chestpain starting at 3AM, radiating to his upper back. He had a history of pulmonary embolism but was no longer on coumadin and states the pain is different. The patient was very hypertensive and had back pain, so they did a CT of his chest to rule out dissection.
Written by Pendell Meyers and Peter Brooks MD A man in his 30s with no known past medical history was reported to suddenly experience chestpain and shortness of breath at home in front of his family. CT angiogram showed extensive saddle pulmonary embolism. He had multiple cardiac arrests with ROSC regained each time.
KEY Point: Although true that patients with longstanding, severe pulmonary disease may manifest a QRST complex in standard lead I with marked overall reduction in QRST amplitude ( See ECG Blog #65 — regarding Schamroth’s Sign ) — you should never normally see a completely flat line in any of the standard limb leads.
There was no chestpain. V1 and V2 are probably placed too high on the chest given close morphological similarity to aVR. The CXR demonstrated no pulmonary edema. The fall was not a mechanical etiology. He denied any specific prodrome of gross palpitations, however did endorse feeling quite dizzy just before the event.
Today’s patient presented to the ED not only with chestpain — but also with shortness of breath , therefore with a history potentially consistent with the diagnosis. For a 10-minute video review on reading Pulmonary CT Scan — WATCH_this_VIDEO by Dr. Jake Gibbons.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










































Let's personalize your content