This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A 50-something male with hypertension and 20- to 40-year smoking history presented with 1 week of stuttering chestpain that is worse with exertion, which takes many minutes to resolve after resting and never occurs at rest. At times the pain does go to his left neck. It is a ssociated with mild dyspnea on exertion.
Written by Willy Frick A man in his 50s with history of hypertension, hyperlipidemia, and a 30 pack-year smoking history presented to the ER with 1 hour of acute onset, severe chestpain and diaphoresis. His ECG is shown: What do you think? What do you think? This was the cost of preventing infarction of the anterior wall.)
A 63 year old man with a history of hypertension, hyperlipidemia, prediabetes, and a family history of CAD developed chestpain, shortness of breath, and diaphoresis after consuming a large meal at noon. He called EMS, who arrived on scene about two hours after the onset of pain to find him hypertensive at 220 systolic.
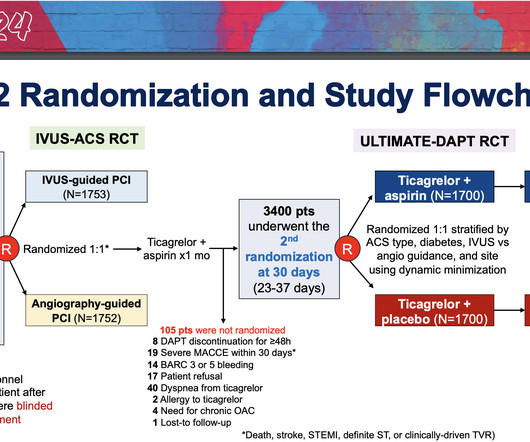
The study focused on patients who underwent PCI for acute coronary syndromes (ACS)—life-threatening conditions which include heart attacks and chestpain caused by decreased blood flow to the heart—with stents containing drugs to prevent further plaque buildup. Stents were supplied by Medtronic Corp.
The patient said his chestpain was 4/10, down from 8/10 on presentation. Although it is statistically unlikely, multiple plaque ruptures are possible. The PDA plaque was also bulky, but was not described as inflamed or ulcerated. The PDA plaque was also bulky, but was not described as inflamed or ulcerated.
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chestpain. He described it as "10/10" intensity, radiating across his chest from right to left. This is written by Willy Frick, an amazing cardiology fellow in St.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chestpain relieved by rest. This episode of chestpain began 3 hours ago and was persistent even at rest. Troponin was ordered.
Written by Willy Frick A 40 year old woman was at home cooking when she developed chestpain. Smith comment : a very high proportion of MINOCA are ruptured plaque with lysed thrombus. That plaque is at risk of thrombosing again. An angiogram is a " lumenogram " and does not "see" the extraluminal plaque.
It means either a percutaneous coronary intervention with a stent or CABG. You may be. But I am not.You need to undergo some re-vascularisation procedure. What do you mean by that Doctor ? Can I get my heart re-vascularised by drugs alone Doctor ? No we can’t. Hmmm , wait, we do have something called OMT/GDMT.
Description of Case:A 64-year-old male with complex medical history, including infective endocarditis of the aortic valve requiring surgical replacement with a bioprosthetic valve and recurrent infective endocarditis of the bioprosthetic valve, presented with two hours of crushing chestpain and found to have ST elevations.
CT coronary angiogram is useful to rule out significant blocks in in those presenting with chestpain to the emergency department. But it may not be that useful just to screen for blocks or build-up of plaques in those without any symptoms. Detection of minor plaques in those persons might lead on to undue anxiety.
No patient with chestpain should be sent home without troponin testing. A chest x-ray in the ED found bilateral pleural effusions. The scan did not find PE, but showed evidence of coronary plaque: There are areas of dense white in the LAD (red and blue circles) and in the first diagonal (green circle).
A 34 yo woman with a history of HTN, h/o SVT s/p ablation 2006, and 5 months post-partum presented with intermittent central chestpain and SOB. She had one episode of pain the previous night and two additional episodes early on morning the morning she presented. Deep breaths are painful and symptoms come and go.
A 40-something woman had sudden chestpain. Today, they viewed the angiogram and concluded that the thrombus at the mid RCA must have extended proximally from the culprit ruptured plaque, extending proximal to the RV marginal branch and temporarily occluding it. He did, found the true culprit, and went back in to stent it.
The lesion was stented. While ST coving in V1 is not necessarily abnormal — the presence of ST elevation in association with ST-T wave abnormalities in V2,V3 in a patient with chestpain is clearly cause for concern. It seems that there was some uncertainly about this. There is also ST coving and elevation in lead V1.
Opened and stented. Acute MI due to plaque rupture does happen in young people, including young women. Instead, in a patient with new chestpain and hyperacute inferior lead T waves — this picture that we see in lead V3 suggests associated posterior OMI until proven otherwise. Beware a low HEART score.
She was treated medically for NonSTEMI, pending next day cath, which showed ulcerated plaque and a 60% thrombotic stenosis in the LAD distal to the first diagonal. It was stented. Echo may be normal ( especially if the patient no longer has chestpain ). Regional wall motion abnormality-distal septum and apex.
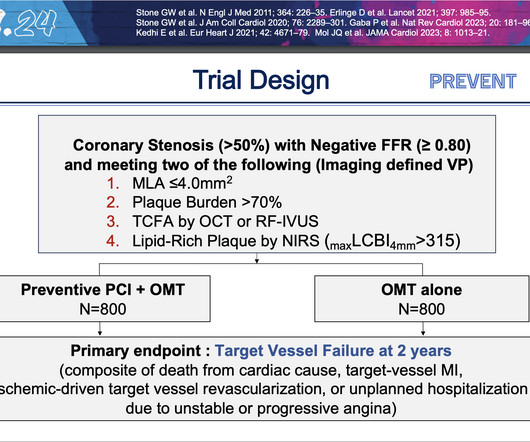
These new findings suggest that people with high-risk plaques that are likely to rupture could benefit from the procedure as a pre-emptive measure rather than waiting for a heart attack or other severe reduction in blood flow to occur. During PCI, an operator inserts a stent into a blocked artery through a catheter in the groin or arm.
Stone, MD Mount Sinai Health System tim.hodson Wed, 04/02/2025 - 15:26 March 31, 2025 Using intravascular imaging (IVI) to guide stent implantation during complex stenting procedures is safer and more effective for patients with severely calcified coronary artery disease than conventional angiography, the more commonly used technique.
Given the presentation, the cardiologist stented the vessel and the patient returned to the ICU for ongoing critical care. He did not remember whether he had experienced any chestpain. (TIMI 3 means the rate of passage of dye through the coronary artery is normal by angiography.) Two subsequent troponins were down trending.
The logic of stenting obstructed coronary arteries is simple. A stent unblocks the artery. Subscribe now Stenting stable coronary artery disease has not been convincingly proven to reduce the risk of future heart attacks or death 1. But coronary stenting is not the only way to reduce symptoms of angina. All is fixed.
One of the most common questions I get is, “ Do I need a stent to treat my heart disease?” ” Typically, several of this person’s friends have had stents, so it seems natural to ask. First, we must understand what a stent is and why it is used. The stent ‘unblocks’ it. Flow is restored.
A CTCA provides much more anatomical detail and can identify advanced plaque often missed by CT Coronary Artery Calcium Score scans alone. Share ChestPain Symptoms There is no role for CT Calcium Scoring in the setting of someone with chestpain symptoms suspected to be from a narrowed coronary artery.
Case A 42-year-old lady presented to the ED with complaints of intermittent episodes of chestpain associated with shortness of breath for the last 2 days. This was her ECG (it is unclear if this was with or without pain): Computerized ECG Read: “Normal sinus rhythm. This case was written by Sam Ghali: ( @EM_RESUS ). Normal ECG.”
This was diagnosed by IVUS (intravascular ultrasound) as a ruptured plaque. It was stented. As there was ruptured plaque, this is NOT Prinzmetal's angina. It is just as dangerous, as there is a ruptured plaque with thrombus (which lysed) in the proximal LAD. Values: STE60V3 = 2.0, QRS V2 = 10, RAV4 = 15.5, Thelin et al.
Case submitted by Andrew Grimes, Advanced Care paramedic, with additions from Jesse McLaren and Smith An 84-year-old male with a notable cardiac history (CABG, multiple stents) woke at 0500hrs with pressure in his chest, diaphoresis, and light-headedness. Influenza-like illness can also trigger plaque rupture.
Written by Willy Frick A 51 year old man with hypertension presented with three hours of acute onset, severe midsternal chestpain associated with two episodes of nausea and vomiting. or 2) Inferior and lateral OMI that is beginning to reperfuse, even though the patient still has chestpain? ECG 1 What do you think?
Written by Willy Frick A young woman with a history of paroxysmal nocturnal hemoglobinuria presented with acute substernal chestpain. The report describes heavy plaque in the proximal RCA by IVUS, but no lesions in the previously occluded RPL branch and no stent was deployed. Smith : The cath lab should be activated now!
A 50 something male presented in the evening to ED for evaluation of chestpain that started at 1600. He reports this was similar to how he felt when he had his heart attack 4 years prior, now s/p 4 stents. The chestpain continued for hours. The patient was still having chestpain.
Written by Willy Frick A woman in her 60s with very severe hyperlipidemia (LDL >200 mg/dL) presented with acute onset chestpain. She described the pain as moderate in severity, and said it had come and gone several times over the next few hours before ultimately resolving. Her symptoms began while getting off the bus.
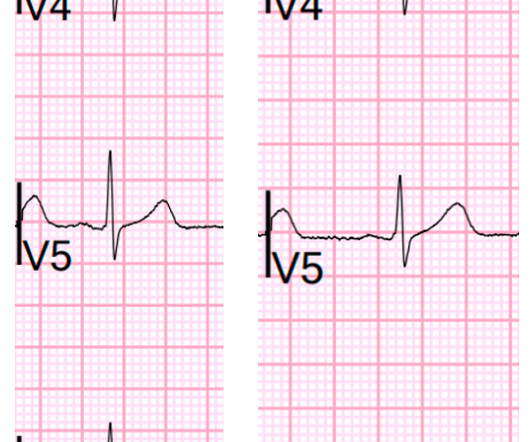
After stent deployment, we often see improvement in the ST-T within seconds or minutes. Here is the final angiogram following placement of a stent in the ostial RCA. 2:04 PM, post stent deployment You can see that even after complete restoration of flow, the ECG still looks terrible, V most of all.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


































Let's personalize your content