This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
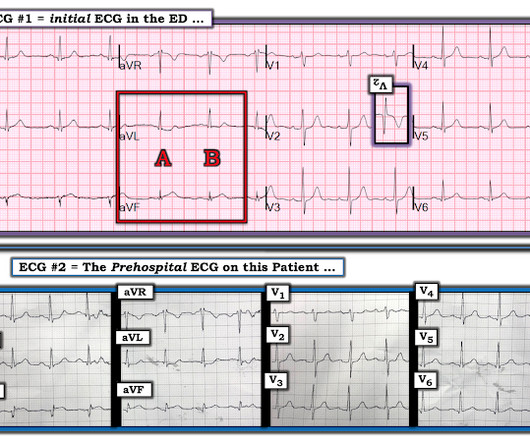
A 50-something male with hypertension and 20- to 40-year smoking history presented with 1 week of stuttering chestpain that is worse with exertion, which takes many minutes to resolve after resting and never occurs at rest. At times the pain does go to his left neck. What do you think the prehospital ECG showed (with pain)?
Written by Willy Frick A man in his 50s with history of hypertension, hyperlipidemia, and a 30 pack-year smoking history presented to the ER with 1 hour of acute onset, severe chestpain and diaphoresis. For national registry purposes, this will be incorrectly classified as a STEMI.) Most STEMI have peak cTnI greater than 10.0.
A 63 year old man with a history of hypertension, hyperlipidemia, prediabetes, and a family history of CAD developed chestpain, shortness of breath, and diaphoresis after consuming a large meal at noon. He called EMS, who arrived on scene about two hours after the onset of pain to find him hypertensive at 220 systolic.
A previously healthy middle-aged male presented shortly after the acute onset of chestpain very shortly before calling 911. On arrival, he was pain free: What do you think? Jerry Jones commented: "Any ST depression on the ECG of a patient with chestpain credible for ACS represents a reciprocal change until proved otherwise."
[link] A 30 year-old woman was brought to the ED with chestpain. She had given birth a week ago, and she had similar chestpain during her labor. She attributed the chestpain to anxiety and stress, saying "I'm just an anxious person." examined SCAD presenting as STEMI (unlike Hassan et al.
Sent by Drew Williams, written by Pendell Meyers A man in his 50s with history of hypertension was standing at the bus stop when he developed sudden onset severe pressure-like chestpain radiating to his neck and right arm, associated with dyspnea, diaphoresis, and presyncope. When is it anterior STEMI? Is this Acute Ischemia?
Shortly after receiving epinephrine, the patient developed new leg cramps and chestpain. The chestpain was described as sharp and radiated to both arms. During active chestpain an ECG was recorded: Meyers ECG interpretation: Sinus tachycardia, normal QRS complex, STD in V2-V6, I, II, III and aVF.
Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. He was given aspirin and sublingual nitro and the pain resolved. Conversely, pathological evaluation, as shown in Fig 2, will correctly identify the percentage of cross-sectional area occupied by plaque. He was started on nitro gtt.
The ECG is diagnostic for acute transmural infarction of the anterior and lateral walls, with LAD OMI being the most likely cause (which has various potential etiologies for the actual cause of the acute coronary artery occlusion, the most common of which is of course type 1 ACS, plaque rupture with thrombotic occlusion).
Despite the absence of significant coronary stenosis on her post-arrest cath — the ECG in Figure-1 is clearly diagnostic of an extensive anterolateral STEMI ( presumably from acute LAD [ L eft A nterior D escending ] coronary artery occlusion). The rhythm in ECG #1 is regular and supraventricular at a rate of ~75/minute.
A 70-something female with no previous cardiac history presented with acute chestpain. She awoke from sleep last night around 4:45 AM (3 hours prior to arrival) with pain that originated in her mid back. She stated the pain was achy/crampy. Over the course of the next hour, this pain turned into a pressure in her chest.
He did not state he had chestpain, but, then again, he couldn't remember anything. This is as clear a STEMI as you can get. So this is classic inferoposterior STEMI on the ECG but is NOT acute coronary syndrome! This 80 year old with a history of CABG had a cardiac arrest.
A 20-something male presented from an outside facility with Chestpain. He came with this ECG from the outside facility, recorded 1 hour after pain onset: There is at least 2 mm of inferior ST elevation, with reciprocal ST depression in aVL, ST flattening in V4-V6, and T-wave inversion in V2. Vital signs were normal.
It does, in fact, the STE meets STEMI criteria since there is 1 mm of in V4 and V5. Here is the clinical story: A 40 year old male with no cardiac history presented with acute substernal chestpain that started 40 minutes prior to arrival. This ECG was texted to me with no other information. What did I say?
This patient, who is a mid 60s female with a history of hypertension, hyperlipidemia and GERD, called 911 because of chestpain. A mid 60s woman with history of hypertension, hyperlipidemia, and GERD called 911 for chestpain. It is also NOT the clinical scenario of takotsubo (a week of intermittent chestpain).
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chestpain. He described it as "10/10" intensity, radiating across his chest from right to left. This is written by Willy Frick, an amazing cardiology fellow in St.
The patient said his chestpain was 4/10, down from 8/10 on presentation. Although it is statistically unlikely, multiple plaque ruptures are possible. The PDA plaque was also bulky, but was not described as inflamed or ulcerated. The PDA plaque was also bulky, but was not described as inflamed or ulcerated.
Here is a case of an 89 year old woman who had syncope but no chestpain or shortness of breath. There was a ruptured plaque with thrombus in the LAD, with some flow still (accounting for the inverted T waves). Learning point: some EKGs represent STEMI no matter what the symptoms, until proven otherwise by angiography.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chestpain relieved by rest. This episode of chestpain began 3 hours ago and was persistent even at rest. Troponin was ordered.
A 34 yo woman with a history of HTN, h/o SVT s/p ablation 2006, and 5 months post-partum presented with intermittent central chestpain and SOB. She had one episode of pain the previous night and two additional episodes early on morning the morning she presented. Deep breaths are painful and symptoms come and go.
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. aVR ST segment elevation: acute STEMI or not? aVR ST Segment Elevation: Acute STEMI or Not?
Could this be Septal STEMI (STE in V1 and aVR, with reciprocal ST depression in V4-V6?), In Septal STEMI , transmural ischemia of the septum is recorded by the overlying lead V1 as ST Elevation. Lead III is also on the right and might manifest ST Elevation in Septal STEMI. with ADDED STE in III?
A 40-something woman had sudden chestpain. This is of course diagnostic of an acute coronary occlusion MI (OMI) that also meets STEMI criteria. Comment by KEN GRAUER, MD ( 7/11/2018 ): = Insightful blog post by Dr. Smith regarding ECG criteria for recognizing acute RV involvement in patients with inferior STEMI.
The chief complaint was "chestpain." Of course, it is actually clearly an acute inferior MI, even though (as is so frequent) it does not meet "STEMI criteria." Male patient: I went back to the room of the first patient and he stated that he had been having chestpain on and off for 3 days. Learning Points 1.
It is equivalent to a transient STEMI. Not much, but studies of STEMI and NonSTEMI show that about 70% of those diagnosed with STEMI have a peak troponin I above 10 ng/mL and that about 70% of those diagnosed with NonSTEMI have a peak troponin I below 10 ng/mL. Again, cath lab was not activated. Take Another Look at Figure-1.
This is why it is essential that the OMI/NOMI paradigm replace the STEMI/NonSTEMI paradigm. Under Non-STEMI, this patient would not have intervention until at least 20 hours (next day), after the infarct is completed. Acute MI due to plaque rupture does happen in young people, including young women. Learning Points: 1.
EMS recorded these prehospital ECGs: Time 0: In V2-V4, there is ST elevation that does not meet STEMI "criteria," of 1.5 She was having a transient STEMI, briefly. It did not progress to full STEMI with loss of the anterior wall, as in this case. Also, persistence of a pain free state does not guarantee an open artery.
No prior exertional complaints of chestpain, dizziness, lightheadedness, or undue shortness of breath. He denied headache or neck pain associated with exertion. 50% of LAD STEMIs do not have reciprocal findings in inferior leads, and many LAD OMIs instead have STE and/or HATWs in inferior leads instead. Pericarditis?
A 40-something male presented with dyspnea and left arm numbness, and perhaps some chest tightness, for 1 1/2 hours. This is all but diagnostic of STEMI, probably due to wraparound LAD The cath lab was activated. This was diagnosed by IVUS (intravascular ultrasound) as a ruptured plaque. Values: STE60V3 = 2.0, It was stented.
Written by Pendell Meyers and Peter Brooks MD A man in his 30s with no known past medical history was reported to suddenly experience chestpain and shortness of breath at home in front of his family. Chestpain, SOB, Precordial T-wave inversions, and positive troponin. What is the Diagnosis? Now another, with ultrasound.
Influenza-like illness can also trigger plaque rupture. STEMI criteria are only 43% sensitive for OMI. He was given two separate sprays of nitroglycerin sublingually, neither of which improved his pain but did cause him to become briefly hypotensive ( 600 ng/L. But in 34% there is persistent occlusion at next day angiogram.
A man in his early 30s was walking when he developed central chestpain which was non-radiating, then had a syncopal event with bowel incontinence, and when he woke up he had ongoing chestpain. Notes never having symptoms like this before, pain is so severe its causing SOB. He called 911. Embolism with lysis.
Written by Willy Frick A young woman with a history of paroxysmal nocturnal hemoglobinuria presented with acute substernal chestpain. The report describes heavy plaque in the proximal RCA by IVUS, but no lesions in the previously occluded RPL branch and no stent was deployed. It is consistent with an inferior LV aneurysm.
Case 1: 20-something woman with chestpain Case 2: 50-something man with chestpain Case 1 A 20-something yo woman presented in the middle of the night with severe crushing chestpain. They also recommended a NTG drip, after which she reported complete resolution of pain. She was a walk-in at triage.
A 50 something male presented in the evening to ED for evaluation of chestpain that started at 1600. Note: the 2022 ACC Expert consensus Chestpain guidelines state that "posterior STEMI-Equivalent" is a sign of acute coronary occlusion. The chestpain continued for hours. NSTEMI-OMI").
Written by Willy Frick A man in his 60s with a history of hypertension and 40 pack-year history presented to the ER with 1 day of intermittent, burning substernal chestpain radiating into both arms as well as his back and jaw. In the world of STEMI, we are incapable of recognizing the first ECG as a false negative.
He denied chestpain. This was attributed to a "Type 2 MI", which is acute MI that is not due to ruptured plaque, but rather due to "supply demand oxygen mismatch". Most MINOCA is due to ruptured plaque with thrombus that lyses and does not leave behind a visible culprit. See these posts: Dynamic OMI ECG.
The fear comes built in with the diagnosis often amplified by young felllows on call (& often times by senior consultants as well) It may appear real, from a clinical angle, but trust, when we deal with the whole gamut of so-called ACS (other than STEMI), there is indeed a benign face in many of them.
He had no chestpain, dyspnea, or any other anginal equivalent, and his vital signs were normal. Mechanisms of plaque formation and rupture. Coronary plaque disruption. Just a few weeks ago, I took care of a patient who had ostial RCA OMI (TIMI 0 at cath) and his only complaint was syncope! link] Bentzon, J.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











































Let's personalize your content