This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Coronary artery spasm (CAS), or Prinzmetal angina, is a recognised cause of myocardial ischaemia in non-obstructed coronary arteries which typically presents with anginal chestpain. The patient presented with recurrent palpitations and pre-syncope, with no chestpain.
A 50-something male with hypertension and 20- to 40-year smoking history presented with 1 week of stuttering chestpain that is worse with exertion, which takes many minutes to resolve after resting and never occurs at rest. At times the pain does go to his left neck. It is a ssociated with mild dyspnea on exertion.
Written by Willy Frick A man in his 50s with history of hypertension, hyperlipidemia, and a 30 pack-year smoking history presented to the ER with 1 hour of acute onset, severe chestpain and diaphoresis. His ECG is shown: What do you think? What do you think? This was the cost of preventing infarction of the anterior wall.)
A 60-something yo female presented w/ exertional chestpain for 3 days. Pain was 8/10 and constant. She has been experiencing progressively worsening exertional dyspnea and chest tightness mostly when climbing up flights of stairs since early September. But the patient has active chestpain.
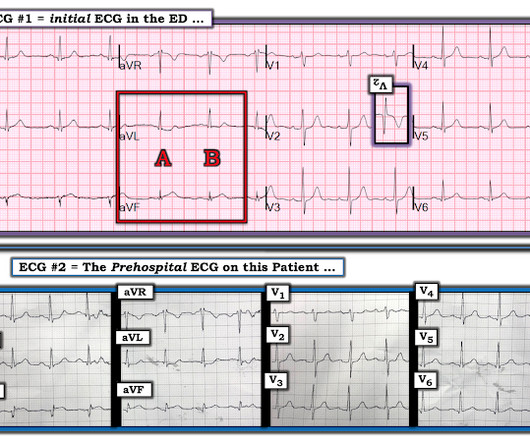
A previously healthy middle-aged male presented shortly after the acute onset of chestpain very shortly before calling 911. On arrival, he was pain free: What do you think? Jerry Jones commented: "Any ST depression on the ECG of a patient with chestpain credible for ACS represents a reciprocal change until proved otherwise."
Artery Damage : Hypertension damages the inner lining of your arteries, making them less elastic and more prone to plaque buildup. Coronary Artery Disease (CAD) : High blood pressure accelerates the development of CAD by promoting the buildup of plaques in the coronary arteries.
[link] A 30 year-old woman was brought to the ED with chestpain. She had given birth a week ago, and she had similar chestpain during her labor. She attributed the chestpain to anxiety and stress, saying "I'm just an anxious person." A similar episode had occurred a week earlier during labor.
Shortly after receiving epinephrine, the patient developed new leg cramps and chestpain. The chestpain was described as sharp and radiated to both arms. During active chestpain an ECG was recorded: Meyers ECG interpretation: Sinus tachycardia, normal QRS complex, STD in V2-V6, I, II, III and aVF.
Sent by Drew Williams, written by Pendell Meyers A man in his 50s with history of hypertension was standing at the bus stop when he developed sudden onset severe pressure-like chestpain radiating to his neck and right arm, associated with dyspnea, diaphoresis, and presyncope. EMS arrived and administered aspirin and nitroglycerin.
Thus, it has recently become generally accepted that most plaque ruptures resulting in myocardial infarction occur in plaques that narrow the lumen diameter by 40% of the arterial cross section may be involved by plaque. The pathologist may see a plaque that constitutes, for example, 50% of the cross-sectional area.
A 63 year old man with a history of hypertension, hyperlipidemia, prediabetes, and a family history of CAD developed chestpain, shortness of breath, and diaphoresis after consuming a large meal at noon. He called EMS, who arrived on scene about two hours after the onset of pain to find him hypertensive at 220 systolic.
15 , 2024 — Four of the seven Medicare Administrative Contractors (MACs) have released final local coverage determinations (LCD) for AI-Coronary Plaque Analysis (AI-CPA). tim.hodson Wed, 10/16/2024 - 12:36 Oct. The four contractors for the U.S.
This is a previously healthy male teenager who was awoken by chestpain. The pain is described as located in the midsternal area, radiating to the right arm, described as 8-9/10 and worse with deep inspirations. In the evening, he became diaphoretic and complained of 9/10 continuous chestpain.
Clinical introduction Vignette A man in his 40s presented to our emergency department with sudden onset of severe central chestpain radiating to his left arm. The left system showed no disease in the left main stem, but mild plaque disease in the dominant left circumflex artery. There was no antecedent angina.
The ECG is diagnostic for acute transmural infarction of the anterior and lateral walls, with LAD OMI being the most likely cause (which has various potential etiologies for the actual cause of the acute coronary artery occlusion, the most common of which is of course type 1 ACS, plaque rupture with thrombotic occlusion). Is there STEMI?
First runner-up for the YIA is Seokhun Yang, MD , of Seoul National University Hospital, for his abstract, “Prognostic Implications Of Coronary CT Angiography-derived Plaque And Hemodynamic Features On Acute Coronary Syndrome Across Varying Time Intervals: Emerald-ii Study.” and the Ma Family, who provided a $5,000 case prize for the winner.
A 20-something male presented from an outside facility with Chestpain. He came with this ECG from the outside facility, recorded 1 hour after pain onset: There is at least 2 mm of inferior ST elevation, with reciprocal ST depression in aVL, ST flattening in V4-V6, and T-wave inversion in V2. Vital signs were normal.
As discussed in detail in ECG Blog #228 — this seemingly qualifies as a “ Silent ” MI ( Approximately half of those MIs not accompanied by CP — have some other associated symptom such as syncope, which substitutes as a “chestpain equivalent” ).
A 70-something female with no previous cardiac history presented with acute chestpain. She awoke from sleep last night around 4:45 AM (3 hours prior to arrival) with pain that originated in her mid back. She stated the pain was achy/crampy. Over the course of the next hour, this pain turned into a pressure in her chest.
In most countries, the pressurised and overcrowded environment of the emergency department serves as the intermediary to discriminate a plaque rupture event from other causes of chestpain. 1 In this.
With more than 500 peer-reviewed publications, the HeartFlow FFR CT Analysis remains unparalleled in precision coronary care, as supported by the ACC/AHA ChestPain Guidelines, to improve treatment plans and outcomes. 2021 ACC/AHA ChestPain Guidelines. said John Farquhar, Chief Executive Officer at HeartFlow.
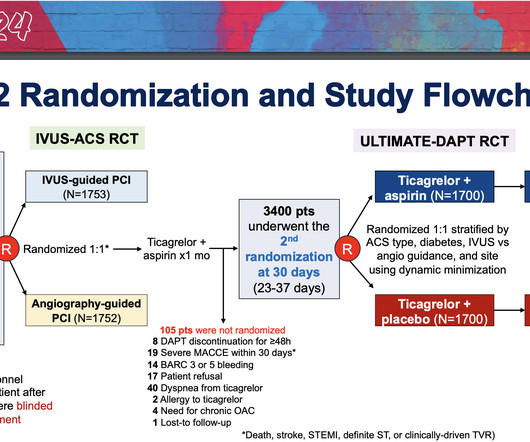
The study focused on patients who underwent PCI for acute coronary syndromes (ACS)—life-threatening conditions which include heart attacks and chestpain caused by decreased blood flow to the heart—with stents containing drugs to prevent further plaque buildup.
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chestpain. He described it as "10/10" intensity, radiating across his chest from right to left. This is written by Willy Frick, an amazing cardiology fellow in St.
He also complained of intermittent mild chestpain radiating into into both shoulders and his back, as well as occasional unexplained sweating. He had no further chestpain. He described mild substernal chestpain, again radiating into both shoulders with occasional sweating. The name is self-explanatory.
Here is the clinical story: A 40 year old male with no cardiac history presented with acute substernal chestpain that started 40 minutes prior to arrival. In spite of a relatively short QTc of 376 ms, the very low R-wave amplitude in V4 and the ST Elevation at 60 ms after the J-point in lead V3 contribute to a high final value.
The patient said his chestpain was 4/10, down from 8/10 on presentation. Although it is statistically unlikely, multiple plaque ruptures are possible. The PDA plaque was also bulky, but was not described as inflamed or ulcerated. The PDA plaque was also bulky, but was not described as inflamed or ulcerated.
There was no chestpain. V1 and V2 are probably placed too high on the chest given close morphological similarity to aVR. Sudden narrowing of a coronary artery due to ACS (plaque rupture with thrombosis and/or downstream showering of platelet-fibrin aggregates). The fall was not a mechanical etiology. Type I ischemia.
This patient, who is a mid 60s female with a history of hypertension, hyperlipidemia and GERD, called 911 because of chestpain. A mid 60s woman with history of hypertension, hyperlipidemia, and GERD called 911 for chestpain. It is also NOT the clinical scenario of takotsubo (a week of intermittent chestpain).
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chestpain relieved by rest. This episode of chestpain began 3 hours ago and was persistent even at rest. Troponin was ordered.
However ,we have some effective clinical and pathological markers too, for effective re-vascularisation They are clinical well being and good functional capacity , relief from chest-pain, reduction of plaque volume, plaque stabilisation, maintenance of collaterals , microvascular patency , reduction of recurrent events.
Written by Willy Frick A 40 year old woman was at home cooking when she developed chestpain. Smith comment : a very high proportion of MINOCA are ruptured plaque with lysed thrombus. That plaque is at risk of thrombosing again. An angiogram is a " lumenogram " and does not "see" the extraluminal plaque.
Sustained inflammation can damage your blood vessels, leading to atherosclerosis (plaque buildup) and increasing your risk of heart attack and stroke. This can lead to chestpain (angina) and increase your risk of heart attack or stroke, especially if you already have underlying heart disease.
She asked me why I felt she had had a heart attack and I explained to her that she had had chestpains and the blood test indicating damage to the heart was elevated and that was all we needed to say that she had had a heart attack. On the basis of these findings we told her that she had suffered a heart attack.
A 34 yo woman with a history of HTN, h/o SVT s/p ablation 2006, and 5 months post-partum presented with intermittent central chestpain and SOB. She had one episode of pain the previous night and two additional episodes early on morning the morning she presented. Deep breaths are painful and symptoms come and go.
Here is a case of an 89 year old woman who had syncope but no chestpain or shortness of breath. There was a ruptured plaque with thrombus in the LAD, with some flow still (accounting for the inverted T waves). Her initial EKG (#1) shows some ST depression in V4-V6, possibly ischemic or possibly due to LVH.
This condition occurs when the blood vessels that supply blood to the heart become blocked or narrowed by plaque buildup. As a result, the heart doesnt receive enough oxygen-rich blood, which can lead to chestpain, shortness of breath, or even a heart attack.
Description of Case:A 64-year-old male with complex medical history, including infective endocarditis of the aortic valve requiring surgical replacement with a bioprosthetic valve and recurrent infective endocarditis of the bioprosthetic valve, presented with two hours of crushing chestpain and found to have ST elevations.
We present a complex case of NSTEMI with multi-vessel coronary artery disease treated with PCI via the Carlino technique.Case Description:A 60-year-old female with a history of hypertension, diabetes mellitus, and ischemic heart disease presented with severe chestpain that radiated to the neck and was associated with nausea and vomiting.
CT coronary angiogram is useful to rule out significant blocks in in those presenting with chestpain to the emergency department. But it may not be that useful just to screen for blocks or build-up of plaques in those without any symptoms. Detection of minor plaques in those persons might lead on to undue anxiety.
IntroductionAtherosclerosis, the hardening and narrowing of the arteries, occurs due to the buildup of plaque on the inner walls of the arteries which can result in reduced blood flow to the organs and tissues. Risk factors such as smoking, chronic kidney disease, and aging can contribute to plaque formation.
He did not state he had chestpain, but, then again, he couldn't remember anything. The ECG and ultrasound could not have been differentiated from acute plaque rupture with occlusion of the RCA. This 80 year old with a history of CABG had a cardiac arrest. There is concordant ST elevation in all inferior leads.
High cholesterol levels – Elevated levels of bad cholesterol can contribute to plaque buildup in your arteries, increasing the risk of heart disease. Routine blood pressure checks are essential to maintaining a healthy heart as high blood pressure often has no symptoms.
A 69‐year‐old woman with a history of lung cancer, hypertension, chronic tobacco use, atherosclerosis, and known calcified plaque at the left carotid bifurcation on dual antiplatelet therapy presented with acute onset of expressive aphasia and right hemiparesis due to acute left CCAO.
The chief complaint was "chestpain." Male patient: I went back to the room of the first patient and he stated that he had been having chestpain on and off for 3 days. It was actually a dissection, not an atherosclerotic plaque rupture. Two Cases Male Patient I was handed this ECG of a 40-something male patient.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.













































Let's personalize your content