This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A 40-something male presented by ambulance with one hour of chestpain that was improving after sublingual nitroglycerine and 325 mg of aspirin, chewed. Here it is: Obvious Inferior Posterior STEMI (+) OMI. Initial troponin was: 3 ng/L We showed that the first troponin in acute STEMI is often negative in at least 27%.
Sent by anonymous, written by Pendell Meyers A man in his 60s presented with acute chestpain with diaphoresis. Diagnosis: Acute non-ST segment elevation MI (Non-STEMI, or NSTEMI) Second troponin returned at around 0200: 15,894 ng/L 0245 (unclear if ongoing pain or not) Inferoposterior (and lateral V5-6) reperfusion findings.
An 80-something year old man with history of metastatic cancer had acute onset of chestpain and called 911. The computer read Anterior STEMI along with RBBB. There is no typical evolution of MI (so BOTH EKG evolution, and troponin, proves there was no acute MI) 2 weeks later, the patient present with acute chestpain again.
Written by Jesse McLaren, with edits from Smith and Grauer A 60 year old with no past medical history presented with two hours of chestpain radiating to the left arm, with normal vitals. But it doesn’t meet STEMI criteria, and was not identified by the computer or the over-reading cardiologist. What do you think?
A man in his mid 60s with history of CAD and stents experienced sudden onset epigastric abdominal pain radiating up into his chest at home, waking him from sleep. He had active chestpain at the time of triage at 0137 at night, with this triage ECG: What do you think? Chest x-ray was normal. Respect physiology.
Written by Pendell Meyers An elderly woman presented with acute onset chestpain and shortness of breath. There is sinus rhythm with minimal STE in V1-V3, not meeting STEMI criteria. The delay between OMI and STEMI sometimes causes unacceptable loss of myocardium or worse.
QOH versions 1 and 2 both say Not OMI, with high confidence, without any clinical context, despite the abnormal STE meeting STEMI criteria. Context: a man in his 40s presented to the emergency department with 1 day of sudden onset chestpain. I sent this to our group without information and Dr. Smith responded: "Not OMI.
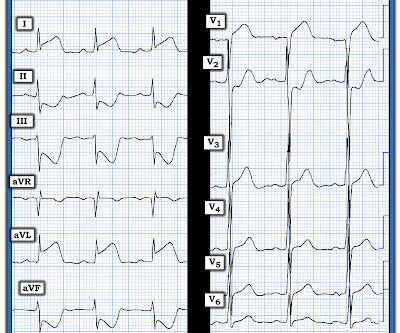
Figure-1: The initial ECG in today's case — obtained from a 50-year old man with new chestpain. ( In contrast — it is EASY to overlook L A- L L reversal — because the ECG picture seen with this type of lead reversal does not immediately stand out as physiologically “off”. How many of these findings can YOU identify?
The patient said his chestpain was 4/10, down from 8/10 on presentation. Additional findings: No ST elevation." Remember that patients with OMI can have normal ECGs! Repeat hsTnI was 183 ng/L, up from 26 ng/L. Around noon, cardiology was called for evaluation. Repeat ECG at that time is shown. ECG 5 Repeat hsTnI rose to 1417 ng/L.
Written by Pendell Meyers and Peter Brooks MD A man in his 30s with no known past medical history was reported to suddenly experience chestpain and shortness of breath at home in front of his family. Chestpain, SOB, Precordial T-wave inversions, and positive troponin. What is the Diagnosis? Now another, with ultrasound.
female with HTN, HLD, diabetes, ESRD on dialysis is brought in by EMS with sudden onset, left -sided chestpain for the past four hours. While she was in her bed at home, she had sudden onset of left sided chestpain that radiated to her shoulder. The pain was pleuritic, without nausea or diaphoresis.
Factors consistently manifesting as such, in addition to chestpain, include, diaphoresis, vomiting, radiation of pain (most alarming when inclusive of both arms), and pain aggravated by exertion. [1] Physiology. Chapter 4: Cardiovascular Physiology. Western Journal of Emergency Medicine, 18 (4), 752-760. [2]
Not quite a STEMI, but same effect.) There is ST elevation in V2-V4 that does not quite meet "STEMI criteria." That is a reasonable thought, but we have shown that if there is one lead of V1-V4 with a T/QRS ratio greater than 0.36, then it is STEMI, not LV aneurysm. Is this a transient STEMI? Is it normal ST elevation?
But lead V2 has a worrisome amount of ST elevation, and in a chestpain patient, I would be worried about STEMI. All bets would be off if instead of no chestpain, this patient had worrisome new-onset symptoms. The Ratios of STE to S-wave: V1: 2.5/16 P EARL : Clinical correlation is KEY in this case.
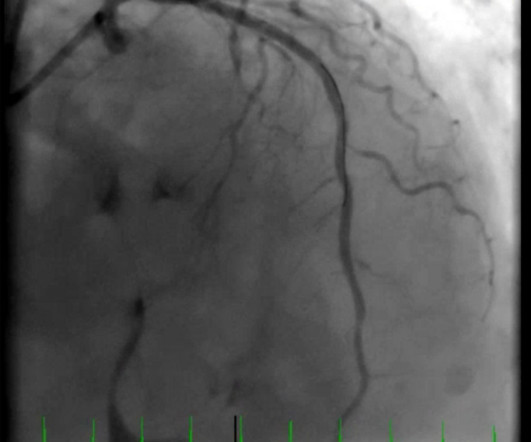
Case A 39-year-old male without prior medical history presents with chestpain that started 2 hours prior to presentation. He says that the pain intensity was 10/10 at home but now about 4/10. Despite the clinical stability and decreasing pain, this patient needs an immediate angiogram. Here are his publications.)
It was edited by Smith CASE : A 52-year-old male with a past medical history of hypertension and COPD summoned EMS with complaints of chestpain, weakness and nausea. Clinical Course The paramedic activated a “Code STEMI” alert and transported the patient nearly 50 miles to the closest tertiary medical center. What do you see?
Written by Pendell Meyers, with edits by Smith A man in his 80s presented with acute chestpain and normal vital signs. It was read by the treating physician and the overreading cardiologist as "Paced, no STEMI." Here is his triage ECG at time = 0: What do you think? (No How does the Queen of Hearts do?
Written by Hans Helseth A 34 year old man with no known medical history presented to the ED after an hour of chestpain. He described the pain as a mid sternal "burning sensation" and rated it 8.5 out of 10 at onset, but on presentation to the ED, reported that the pain had improved to 4.5. 10 chestpain.
He had no chestpain, dyspnea, or any other anginal equivalent, and his vital signs were normal. Given the immediate physiologic chain reaction of intense autonomic dysfunction that followed on learning of her husband's death ( and which ultimately led to this patients demise ) I have to wonder WHEN ( and How? )
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
























Let's personalize your content