This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A 40-something male presented by ambulance with one hour of chestpain that was improving after sublingual nitroglycerine and 325 mg of aspirin, chewed. Here is his initial ED ECG: What do you think? This is because IF the history is recent CP — then this initial ED ECG has to be interpreted like Drs.
Sent by anonymous, written by Pendell Meyers A man in his 60s presented with acute chestpain with diaphoresis. The Importance of the History: As noted above — the onset of chestpain in today's case was acute. He had received aspirin and nitroglycerin by EMS, with some improvement. His vitals were within normal limits.
A 60 year old with chestpain presented to the ED. In this case, lead I does not look bizarre, but all other leads do. == N OTE : The reasons I especially liked today's case are: i ) The patient presented with chestpain — so the importance of distinguishing artifact from reality can not be overstated! —
An elderly woman presented with chestpain that radiated to the back for several hours. The first troponin returned at 0.099 ng/mL (elevated, consistent with Non-Occlusion MI) Providers were concerned with aortic dissection, so they order a chest aorta CT. Here is here initial ECG: There is only a nonspecific flat T-wave in aVL.
Written by Jesse McLaren, with edits from Smith and Grauer A 60 year old with no past medical history presented with two hours of chestpain radiating to the left arm, with normal vitals. Unfortunately, the reality is — that many ( most ) WPW patients who present with chestpain do not manifest intermittent preexcitation.
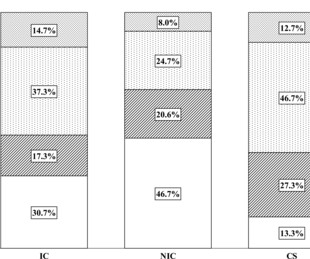
Availability of systematic coronary physiology might result in more homogeneous interpretation and management strategy compared with ICA alone. Methods 150 coronary angiograms from patients with stable chestpain were presented independently to three NICs, three ICs and three CSs. Trial registration number NCT01070771.
An 80-something year old man with history of metastatic cancer had acute onset of chestpain and called 911. There is no typical evolution of MI (so BOTH EKG evolution, and troponin, proves there was no acute MI) 2 weeks later, the patient present with acute chestpain again. He ruled out for MI by troponins again.
5 Revascularization to improve blood flow to the heart has been shown to reduce mortality in stable chestpain patients. 5 Revascularization to improve blood flow to the heart has been shown to reduce mortality in stable chestpain patients. The Lancet, vol. 10390, May 2023, pp. 1798–1809, [link]. Circulation, vol.
Together, the two companies will work to further the development and commercialization of Medis Quantitative Flow Ratio (Medis QFR), a non-invasive approach to the assessment of coronary physiology, as part of GE HealthCare’s interventional cardiology portfolio built around the Allia Platform.
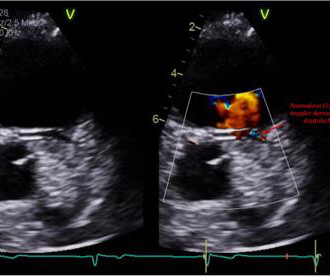
Treadmill exercise stress test showed excellent functional capacity without exercise-induced chestpain or ischemic ECG changes. The RCA demonstrated a normal course to the right atrioventricular groove, and the posterior descending artery arose from the RCA.
Impression: In this middle-aged man with palpitations and dyspnea, but no chestpain — I suspect that the T wave peaking and slight, upward-sloping chest lead ST elevation represent a repolarization variant.
A man in his mid 60s with history of CAD and stents experienced sudden onset epigastric abdominal pain radiating up into his chest at home, waking him from sleep. He had active chestpain at the time of triage at 0137 at night, with this triage ECG: What do you think? Respect physiology.
Context: a man in his 40s presented to the emergency department with 1 day of sudden onset chestpain. Serial echo monitoring showed increasing pericardial pressures without overt tamponade physiology. I sent this to our group without information and Dr. Smith responded: "Not OMI. Pericarditis maybe."
Written by Pendell Meyers and Peter Brooks MD A man in his 30s with no known past medical history was reported to suddenly experience chestpain and shortness of breath at home in front of his family. Chestpain, SOB, Precordial T-wave inversions, and positive troponin. What is the Diagnosis? Now another, with ultrasound.
The patient said his chestpain was 4/10, down from 8/10 on presentation. Additional findings: No ST elevation." Remember that patients with OMI can have normal ECGs! Repeat hsTnI was 183 ng/L, up from 26 ng/L. Around noon, cardiology was called for evaluation. Repeat ECG at that time is shown. ECG 5 Repeat hsTnI rose to 1417 ng/L.
They were recorded 12 minutes apart: "Hey Steve, 30-something with one week of chestpain, mostly right-sided, better with sitting up.": I learned more about the history: 30-something African American with 5-7days of sharp R-sided shoulder/scapula/chest discomfort, presented with sinus tachycardia. What do you think?
female with HTN, HLD, diabetes, ESRD on dialysis is brought in by EMS with sudden onset, left -sided chestpain for the past four hours. While she was in her bed at home, she had sudden onset of left sided chestpain that radiated to her shoulder. The pain was pleuritic, without nausea or diaphoresis.
Men typically experience classic symptoms like chestpain or pressure, radiating down the left arm. Traditional diagnostic tests like electrocardiograms (ECG) and stress tests may not always detect heart issues in women due to variations in their symptoms and heart physiology. However, women may not exhibit these telltale signs.
She asked me why I felt she had had a heart attack and I explained to her that she had had chestpains and the blood test indicating damage to the heart was elevated and that was all we needed to say that she had had a heart attack. Genetics and physiological stress are also risk factors.
Factors consistently manifesting as such, in addition to chestpain, include, diaphoresis, vomiting, radiation of pain (most alarming when inclusive of both arms), and pain aggravated by exertion. [1] Physiology. Chapter 4: Cardiovascular Physiology. Western Journal of Emergency Medicine, 18 (4), 752-760. [2]
Wellens' is a syndrome of a painless period following an anginal (chestpain) event. Chestpain, SOB, Precordial T-wave inversions, and positive troponin. She also complained of generalized weakness, lightheadedness, diaphoresis, chestpain, and cough. What is the Diagnosis?
AV synchrony and physiologic ventricular depolarization the hemodynamics improved. Lowering the back up rate (LRL) of the ICD/pacer allowed for an intrinsic rhythm with physiologic AV conduction and normal AV synchrony with resultant increase in stroke volume and cardiac outpt.
There was no chestpain. The physiologic reason for this — is thought to be the result of momentarily increased circulation from mechanical contraction arising from the "sandwiched in" QRS complex. This was written by Magnus Nossen The patient is a female in her 50s. She presented with a one week hx of «dizziness» and weakness.
And some similar ECGs from Pulmonary Embolism: A young woman with altered mental status and hypotension An elderly woman transferred to you for chestpain, shortness of breath, and positive troponin - does she need the cath lab now? It just doesn’t make physiologic sense to have deep T wave inversion in V1 and V3, but not in V2.
Written by Pendell Meyers An elderly woman presented with acute onset chestpain and shortness of breath. EMS showed us their ECG on arrival at her house: What do you think? There is sinus rhythm with minimal STE in V1-V3, not meeting STEMI criteria.
But lead V2 has a worrisome amount of ST elevation, and in a chestpain patient, I would be worried about STEMI. All bets would be off if instead of no chestpain, this patient had worrisome new-onset symptoms. The Ratios of STE to S-wave: V1: 2.5/16 P EARL : Clinical correlation is KEY in this case.
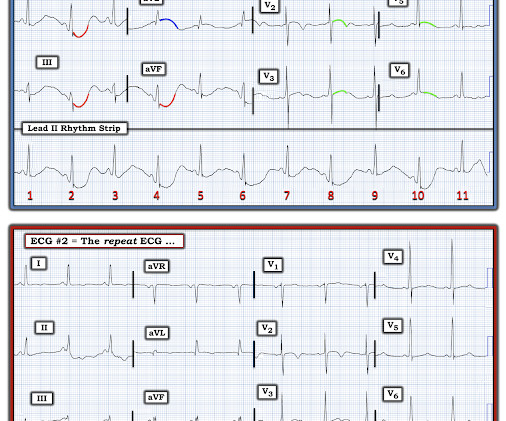
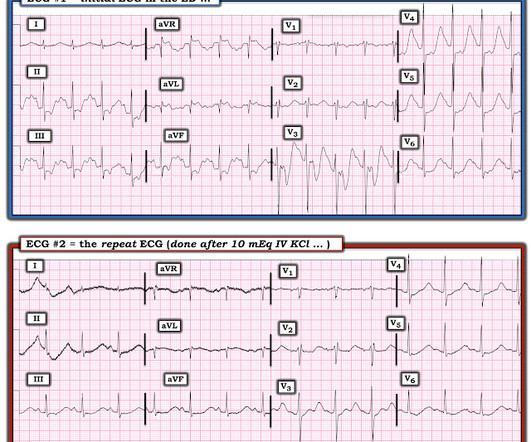
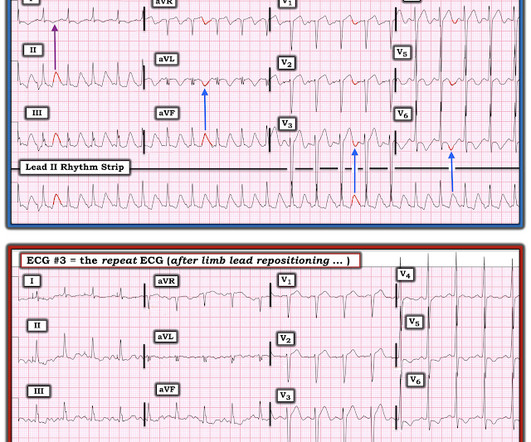
The patient had come to the ED for SOB, but without any chestpain. Other cases of Pulse Tapping Artifact: Acute chestpain and a bizarre ECG Bizarre (Hyperacute??) Therefore, as many as 11 of the 12 leads can look bizarre. Solution : repeat the ECG, but move the left leg electrode. He had a 10 pound weight loss.
Figure-1: The initial ECG in today's case — obtained from a 50-year old man with new chestpain. ( In contrast — it is EASY to overlook L A- L L reversal — because the ECG picture seen with this type of lead reversal does not immediately stand out as physiologically “off”. How many of these findings can YOU identify?
There was no chestpain. Acute posterior OMI would be a prime concern for the ECG in Figure-1 — IF the patient presented with cardiac-sounding chestpain. But today's patient had no chestpain. I was worried that the ST depression and T-wave inversion in V2 and V3 might be posterior OMI.
Case A 39-year-old male without prior medical history presents with chestpain that started 2 hours prior to presentation. He says that the pain intensity was 10/10 at home but now about 4/10. Despite the clinical stability and decreasing pain, this patient needs an immediate angiogram. Here are his publications.)
Acute chestpain and a bizarre ECG Bizarre (Hyperacute??) Electrocardiology 40: 475-477, 2007 ) — which is the BEST review I’ve seen on the physiology explaining the relative size of artifact deflections when the cause of the artifact is from a single extremity. What do you think?
History : An extremely elderly patient who lived independently presented with acute "oppressive" chestpain 7/10 in severity that was not positional, pleuritic, or reproducible. This T wave progression sequence does not make physiologic sense. What's the story?" Exam was benign and VS were normal.
Written by Pendell Meyers, with edits by Smith A man in his 80s presented with acute chestpain and normal vital signs. We need more such ECGs for training but we are constantly working on the algorithm and one day it will make this diagnosis. == But isn't ongoing chestpain in NSTEMI a guideline indication for emergent angiography?
It was edited by Smith CASE : A 52-year-old male with a past medical history of hypertension and COPD summoned EMS with complaints of chestpain, weakness and nausea. Any alteration in physiology can change "compensated" AS to "decompensated" AS. The paramedic’s initial impression of the patient was that he was critically ill.
Real-World Solutions: A Holistic Patient Case Study A 62-year-old woman with diabetes, hypertension, obesity, and a history of depression and trauma presents with chestpain. After a normal stress test, coronary physiology testing revealed endothelial dysfunction with coronary vasospasm.
Check : [vitals, SOB, ChestPain, Ultrasound] If the patient has Abdominal Pain, ChestPain, Dyspnea or Hypoxemia, Headache, Hypotension , then these should be considered the primary chief complaint (not syncope). Aortic Dissection, Valvular (especially Aortic Stenosis), Tamponade.
Written by Hans Helseth A 34 year old man with no known medical history presented to the ED after an hour of chestpain. He described the pain as a mid sternal "burning sensation" and rated it 8.5 out of 10 at onset, but on presentation to the ED, reported that the pain had improved to 4.5. 10 chestpain.
Written by Willy Frick with edits by Ken Grauer An older man with a history of non-ischemic HFrEF s/p CRT and mild coronary artery disease presented with chestpain. He said he had had three episodes of chestpain that day while urinating. ECG 1 What do you think? There is a lot going on in this ECG.
The data show the HeartFlow platform provides clinicians with the insights needed to anticipate and mitigate adverse events, including myocardial infarctions, in symptomatic patients with stable chestpain. The data were presented at the 36th annual Transcatheter Cardiovascular Therapeutics conference in Washington, D.C.
He had no chestpain, dyspnea, or any other anginal equivalent, and his vital signs were normal. Given the immediate physiologic chain reaction of intense autonomic dysfunction that followed on learning of her husband's death ( and which ultimately led to this patients demise ) I have to wonder WHEN ( and How? )
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.







































Let's personalize your content