This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Written by Jesse McLaren, with comments from Smith and Grauer A 60 year old presented with three weeks of intermittent non-exertional chestpain without associated symptoms. A prospective validation of the HEART score for chestpain patients at the emergency department. Backus BE, Six AJ, Kelder JC, et al.
In about 70 percent of cases, patients with HCM experience obstruction to blood flow, which increases pressures in the heart and can lead to chestpain, shortness of breath and reduced exercise capacity.
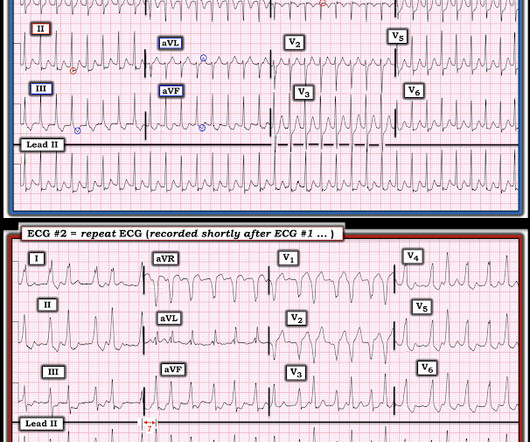
A 30-something presented with chestpain, palpitations, and SOB. Cardioversion can be done pharmacologically (usually procainamide) , but why would you want to do that? He has had similar symptoms for 4 years, but has never been evaluated. This means NO calcium channel blocker, beta blocker, adenosine, or digoxin.
The supposition that beta blockade in the presence of cocaine intoxication would lead to unopposed alpha constriction is not based in accurate pharmacology, and the study that showed this effect with human intracoronary administration was done, as mentioned in the article, with propranolol, a nonselective beta blocker. Marcus, G. Gibler, W.
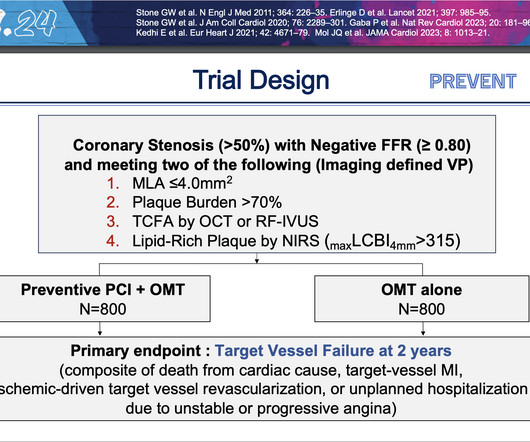
At two years, people who underwent preventive PCI were 89% less likely to experience the composite primary endpoint of cardiac death, heart attack in the target vessel, revascularization due to ischemia in the target vessel or hospitalization for unstable or progressive chestpain compared with people who received medications alone.
24 will focus on the following three current guideline updates: American College of Cardiology (ACC)/American Heart Association (AHA) Guidelines 2023 Atrial Fibrillation Guideline - Pharmacology II: Strokes vs. Bleeds, What Do the Guidelines Tell Us About Practical Management in A-fib? The Guidelines Sessions at ACC.24
New HCM Guidelines Updated recommendations in the guideline reflect recent evidence about HCM treatment and management including new forms of pharmacologic management; participation in vigorous recreational activities and competitive sports; and risk stratification for sudden cardiac death (SCD) with an emphasis on pediatric patients.
A 50-something presented with epigastric and chestpain. Epigastric pain, Syncope, and Saddleback ST Elevation A 65 Year Old Man with Chestpain and Precordial ST Elevation Non-Vagal Syncope and Saddleback Morphology in V2 Is this STEMI? Here is his ECG: What do you think? QTc 388 ms. wave in V1??
A late middle-aged man presented with one hour of chestpain. Crit Care Med 1991; 19:694) Concentrated Potassium Chloride Infusions in Critically Ill Patients with Hypokalemia The Journal of Clinical Pharmacology. Most recent echo showed EF of 60%. He also had a history of chronic kidney disease, stage III.
It was edited by Smith CASE : A 52-year-old male with a past medical history of hypertension and COPD summoned EMS with complaints of chestpain, weakness and nausea. This was contributed by some folks at Wake Forest: Jason Stopyra, Shannon Mumma, Sean O'Rourke, and Brian Hiestand.
Given her reported chestpain, shortness of breath, and syncope, an ECG was quickly obtained: What do you think? This may result from fluctuations in heart rate or in nervous system activity or from pharmacologic treatment. She was noted to be tachycardic and her heart sounds were distant on physical exam.
Results revealed that women are twice as likely to exhibit myocardial ischemia in response to mental stress compared to traditional stressors like exercise or pharmacologic stress. Combining behavioral and pharmacological treatment is most effective. Moreover, women under 50 years old are four times more likely to experience MSIMI.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.















Let's personalize your content