This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
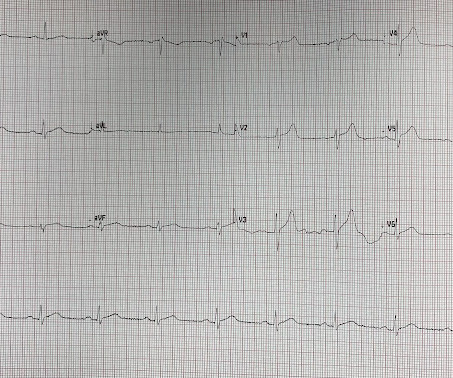
Written by Willy Frick A 67 year old man with a history of hypertension presented with three days of chestpain radiating to his back. This ECG together with these symptoms is certainly concerning for OMI, but the ECG is not fully diagnostic, and another consideration could be acute pericarditis. What do you think?
Acute pericarditis (AP) is the second most common cardiac cause of chestpain, diagnosed when at least two of the following criteria are met: characteristic pleuritic chestpain, pericardial rub on auscultation, new typical ECG changes (such as widespread ST-elevation or PR-depression) and pericardial effusion on imaging.
Written by Pendell Meyers Two patients with acute chestpain. Patient 1: Patient 2: Patient 1: A man in his 40s with minimal medical history presented with acute chestpain radiating to his R shoulder. Two patients with chestpain. Do either, neither, or both have OMI and need reperfusion?
Written by Jesse McLaren, with a very few edits by Smith A 60-year-old presented with chestpain. Inferior hyperacute T waves, which have been added to the 2022 ACC consensus on chestpain as a “STEMI equivalent”[3] 3. ST depression in lead AVL differentiates inferior ST-elevation myocardial infarction from pericarditis.
By Magnus Nossen This ECG is from a young man with no risk factors for CAD, he presented with chestpain. The patient is a young adult male with chestpain. The chestpain was described as pressure like and radiation to both arms and the jaw. It is easy to say pericarditis in such a case.
A healthy 45-year-old female presented with chestpain, with normal vitals. The computer interpretation was “ST elevation, consider early repolarization, pericarditis or injury.” The final cardiology interpretation confirmed the computer interpretation of “ST elevation, consider early repolarization, pericarditis or injury”.
Written by Magnus Nossen with Edits by Grauer and Smith The ECGs in today’s case are from 3 different patients all presenting with new-onset CP ( ChestPain ). These latter findings are typical of pericarditis, but pericarditis never has reciprocal ST depression. This is OMI until proven otherwise.
The patient was discharged with a diagnosis of acute pericarditis — and treated with a full course of colchicine and ibuprofen. The ultimate discharge diagnosis was acute pericarditis. ( From the information provided — I would not make the diagnosis of acute pericarditis. Figure-1: The initial ECG in today's case.
Case An 82 year old man with a history of hypertension presented to the ED with chestpain at 1211. He described his chestpain as pleuritic and reported that it started the day prior while swinging a golf club. His pain suddenly became much worse in the ED and he became acutely diaphoretic, dizzy, and hypotensive.
Jesse McLaren guides us through 9 cases and explains how pericarditis is a diagnosis of exclusion through 3 simple steps: 1. Exclude more serious causes of chestpain, eg wraparound LAD occlusion, inferior OMI 2. Exclude complications of pericarditis, eg myocarditis, large pericardial effusion 3.
A middle-aged patient with lung cancer had presented to clinic complaining of generalized malaise, cough, and chestpain. Symptoms other than chestpain (malaise, cough in a cancer patient) 2. PR depression, which suggests pericarditis 4. Here is that ECG: What do you think? There is sinus tachycardia.
Overall, this looks like one of the rare ECGs that is actually specific for pericarditis in my opinion. Pericarditis maybe." Context: a man in his 40s presented to the emergency department with 1 day of sudden onset chestpain. Meyers' words — "is one of the rare ECGs that is actually specific for pericarditis".
Written by Pendell Meyers A man in his late 40s with several ACS risk factors presented with a chief complaint of chestpain. Several hours prior to presentation, while driving his truck, he started experiencing new central chestpain, without radiation, aggravating/alleviating factors, or other associated symptoms.
It is not always possible to be certain about the origin of chestpain just by its characteristics as the variation between individuals is quite a bit. A medical opinion should be sought in case of any significant chestpain so that important ailment is not missed. A pain lasting more than 30 minutes is usual.
DALLAS, June 17, 2024 — About 40,000 people in the United States experience recurrent pericarditis, or inflammation of the sac-like structure that protects the heart, which can cause chestpain and may lead to fluid buildup around the heart muscle.
Sent by Dan Singer MD, written by Meyers, edits by Smith A man in his late 30s presented with acute chestpain and normal vitals except tachycardia at about 115 bpm. Dr. Singer sent this to me with just the information: "~40 year old with acute chestpain". Acute pain?" -(Dr. I immediately responded: "cool fake!
Healthy male under 25 years old with a pretty good story for acute onset crushing chestpain relieved with nitro. First, many on Twitter said "Pericarditis". This is NOT pericarditis, which virtually NEVER has ST depression any where except aVR. Angiogram : "Acute onset chest pressure with diaphoresis." "ECG
Background There are limited data on acute pericarditis according to different age groups. The aim of this study is to investigate the role of age-related features in clinical characteristics, management, and outcomes of acute pericarditis, with a focus on the geriatric population. Results A total of 471 patients (median age 56.3 (IQR
A 40 something woman with a history of hyperlipidemia and additional risk factors including a smoking history presented with substernal chestpain radiating to "both axilla" as well as the upper back. She was reportedly "pacing in her room while holding her chest". Clinician and EKG machine read of acute pericarditis.
This is a previously healthy male teenager who was awoken by chestpain. The pain is described as located in the midsternal area, radiating to the right arm, described as 8-9/10 and worse with deep inspirations. In the evening, he became diaphoretic and complained of 9/10 continuous chestpain.
Post op chestpain Typical of post-op pericarditis (postpericardiotomy syndrome) There is ST Elevation in II > III, and STE in V3-5, but with flat T-wave. The ST elevation is far more prominent than the T-wave and this is what I see as the defining feature differentiating OMI from pericarditis.
This is a value typical for a large subacute MI, n ormal value 48 hours after myocardial infarction is associated with Post-Infarction Regional Pericarditis ( PIRP ). As already mentioned, this patient could have post-infarction regional pericarditis from a large completed MI. Sinus tachycardia has many potential causes. Hammill SC.
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chestpain similar to his prior MI, but worse. The pain initially started the day prior to presentation. The ST elevation from today is ~0.2
Although generally associated with a favorable safety profile, some patients develop post-procedural positional or pleuritic chestpain that may reflect acute pericarditis. However, the prevalence and clinical significance of this phenomenon remain unclear.
A young otherwise healthy man presented with 4 hours of sharp 10/10 substernal chestpain. But there was some doubt as to whether it might be pericarditis because of the ST elevation in I and II, without ST depression in III. This is a good sign for myocardial infarction and does not happen in pericarditis. BP was 160.
In this ECG Cases blog we look at 10 cases of patients with chestpain, including false positive STEMI, false negative STEMI, and other causes to help hone your ECG interpretation skills in time-sensitive cases where those very ECG skills might save a life.
Pericarditis refers to inflammation of the pericardium The pericardium is a sac within which the heart sits. Acute inflammation of this sac is known as acute pericarditis. About 5% of patients who present to A+E with chestpain which is not deemed to be a heart attack or angina are ultimately diagnosed with pericarditis.
An 80-something year old man with history of metastatic cancer had acute onset of chestpain and called 911. There is no typical evolution of MI (so BOTH EKG evolution, and troponin, proves there was no acute MI) 2 weeks later, the patient present with acute chestpain again. He ruled out for MI by troponins again.
Here is his initial ED ECG: The R-wave in V4 extends to 33 mm, the computerized QTc is 372 ms The only available previous ECG is from one year ago, during the admission when he was diagnosed with pericarditis: 1 year ago ECG, with clinician and computer interpretatioin of pericarditis Normal 0 false false false EN-US X-NONE X-NONE What do you think?
Upon questioning patient, he denies having any chestpain or chest tightness of any sort. Assessment:" " Nonspecific ST elevation from V1-V4 , question of early repolarization versus pericarditis , question of acute current of injury and ? Pericarditis would be even more unlikely in someone without chestpain.
Written by Pendell Meyers, with edits by Steve Smith A man in his early 40s with history of MI s/p PCI presented with bilateral anterior chestpain described as burning and belching with no radiation since last night starting around 11pm (roughly 11 hours ago). The patient was still with ongoing chestpain at the time ECG #1 was done.
He presented to the ED because he developed sudden severe, sharp, pleuritic (but not positional), substernal and left mid to lower chestpain. It could also be due to pericarditis or myocarditis, but I always say that "you diagnose pericarditis at your peril." Pericarditis? Learning Points: 1. What happens then?
Below is the first ECG, signed off by the over-reading cardiologist agreeing with the computer interpretation: ST elevation, consider early repolarization, pericarditis, or injury. Theres ST elevation in V3-4 which meets STEMI criteria, which could be present in either early repolarization, pericarditis or injury. What do you think?
Submitted and written by Quinton Nannet, MD, peer reviewed by Meyers, Grauer, Smith A woman in her 70s recently diagnosed with COVID was brought in by EMS after she experienced acute onset sharp midsternal chestpain without radiation or dyspnea. She felt nauseous and lightheaded with no neurologic deficits.
A 30-something woman with chestpain and h/o pulmonary hypertension due to chronic pulmonary emboli A 30-something with 8 hours of chestpain and an elevated troponin Syncope, Shock, AV block, Large RV, "Anterior" ST Elevation. Chestpain, SOB, Precordial T-wave inversions, and positive troponin.
He reports significant chestpain at the base of his scapula on the right side along with new shortness of breath. Wellen's waves indicate that, when the patient was having chestpain, there was occlusion. See these casese (and I have many others): First ED ECG is Wellens' (pain free). A 70-something y.o.
A physician caring for his new arrival, a 50-something with acute chestpain and dyspnea and syncope, texted me this initial ED ED ECG. ECG Diagnosis: Normal variant ST Elevation vs. Pericarditis. Uncertain whether there is pericarditis or normal variant. No active chestpain 2. What do you think?
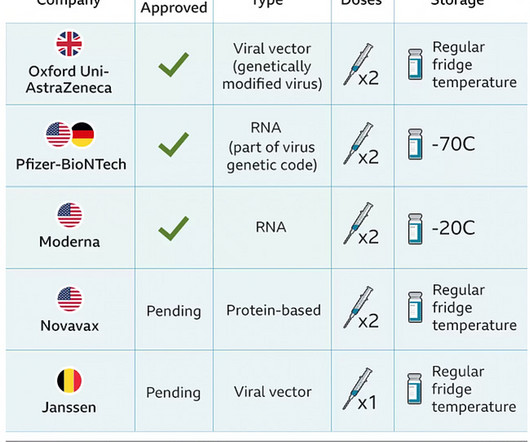
The case reports Case 1 involves a 26 year old man who developed pericarditis after the Pfizer vaccine. Pericarditis, an inflammation of the sac the heart lives in, developed about 7 days after the Pfizer vaccine. The diagnosis was made based on classic findings of inflammation on an electrocardiogram associated with acute chestpain.
3 hours prior to calling 911 he developed typical chestpain. This rules out pericarditis, which essentially never has reciprocal ST depression. This is not pericarditis because: a. Pain was typical for MI (substernal, not postional or sharp, resolved with NTG) b. Pericarditis does not have reciprocal depression.
Myocarditis and pericarditis are inflammatory conditions of the heart that present a range of symptoms, often including chestpain, fatigue, breathlessness and palpitations that may be irregular due to cardiac rhythm disturbances.
Postablation chestpain consistent with pericarditis was reduced with colchicine (4% versus 15%; HR, 0.26 [95% CI, 0.09–0.77];P=0.02) Colchicine did not prevent atrial arrhythmia recurrence at 2 weeks (31% versus 32%; hazard ratio [HR], 0.98 [95% CI, 0.59–1.61];P=0.92) 2.02];P=0.89). 11.53];P<0.001). 1.99];P=0.55).CONCLUSIONS:Colchicine
There are other tests also for tuberculous pericarditis, but they not as sure as growing the bacterium in culture. Inflammation of pericardium as inflammation elsewhere can be painful and cause chestpain. But pericardial effusion can build up slowly without much pain.
Written by Pendell Meyers Two adult patients in their 50s called EMS for acute chestpain that started within the last hour. Of course the patient was saddled with the erroneous "pericarditis" diagnosis after CTs ruled also ruled out PE and dissection. Both were awake and alert with normal vital signs. What do you think?
Written by Pendell Meyers, edits by Smith: Case A 72 year old female with hypertension and COPD presented with sudden shortness of breath and chestpain. A new right bundle branch block in a sick patient with chestpain and/or shortness of breath is a worrisome finding concerning for LAD occlusion or significant pulmonary embolism.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












































Let's personalize your content