This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The post EM Quick Hits 50 Normal Unenhanced CT Renal Colic DDx, Perichondritis, Magnesium in Pediatric Asthma, Steroids for Pneumonia, OMI Cath Lab Activation appeared first on Emergency Medicine Cases.
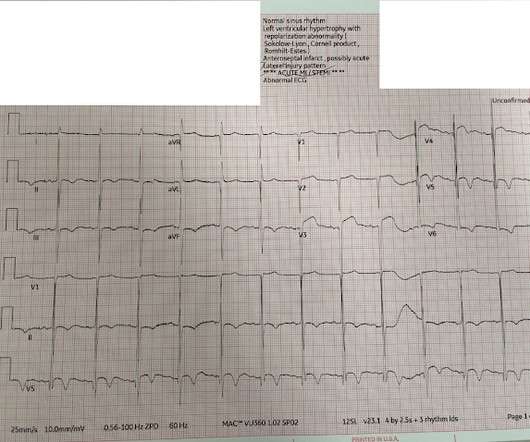
This is a previously healthy male teenager who was awoken by chestpain. The pain is described as located in the midsternal area, radiating to the right arm, described as 8-9/10 and worse with deep inspirations. In the evening, he became diaphoretic and complained of 9/10 continuous chestpain.
There was apparently no syncope and he had no bony injuries, but he did complain of left sided chestpain. His chest was tender. A bedside cardiac ultrasound was normal. An ECG was recorded: Avinash was understandably confused by this ECG. He wrote: "ECG 1 - shows wide ???IVCD IVCD type rhythm ??
He denied chestpain or shortness of breath. In the clinical context of weakness and fever, without chestpain or shortness of breath, the likelihood of Brugada pattern is obviously much higher. Pediatric and elderly patients were more predisposed to developing an arrhythmic event in the setting of fever [7].
The guideline, according to a written statement shared here, reiterates the importance of collaborative decision-making with patients who have HCM and provides updated recommendations for the most effective treatment pathways for adult and pediatric patients. Several recommendations in the new guideline extend to pediatric patients.
The diagnosis was made based on classic findings of inflammation on an electrocardiogram associated with acute chestpain. 2-3 days after this he developed the same sharp chestpain and shortness of breath with elevated inflammatory markers (CRP) as well as typical findings of pericarditis seen on ECG.
There was no chestpain. This was written by Magnus Nossen The patient is a female in her 50s. She presented with a one week hx of «dizziness» and weakness. She was feeling fine prior to the last seven days. She did admit to shortness of breath on exertion. She had no known heart condition.
Note, Denmark stopped recommending the covid vaccine for children <18 years mid summer 2022, dropped all pandemic restrictions 2/2022 including masks (never masked <12) and has had ZERO pediatric deaths due to omicron. Instead, we have had zero pediatric deaths from Omicron. Almost a million followers now.
It was from a patient with chestpain: Note the obvious Brugada pattern. Pediatric and elderly patients were more predisposed to developing an arrhythmic event in the setting of fever [7]. The elevated troponin was attributed to either type 2 MI or to non-MI acute myocardial injury. There is no further workup at this time.
the optimum QT correction formula for patients with chestpain was found to be unique for each individual ; it is a correction factor that can be calculated real-time for each patient by taking multiple measurements over a range of heart rates. Other Research: According to this study b y Batchvarov et al. ,
Acute coronary syndrome in a pediatric patient? days of chestpain that started as substernal and crushing in nature awakening him from sleep and occasionally traveling to right side of neck. The pain was described as constant, worse with deep inspiration and physical activity, sometimes sharp. World J Pediatr.
The patient denied any chestpain whatsoever, and a troponin at zero and 2 hours were both undetectable. Types 2 and 3 have been merged into Type 2 and look substantially different. Is this Type 2 Brugada syndrome/ECG pattern? This was recorded about 30 minutes later: Same A previous ECG was obtained and was normal.
She did not even need to ask in this case, because even if the patient presented with chestpain, she would call it NEGATIVE. Fortunately, the physicians seeing the patient were using the Queen of Hearts PM Cardio AI ECG OMI Model, and she had absolutely no concerns.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

















Let's personalize your content