This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
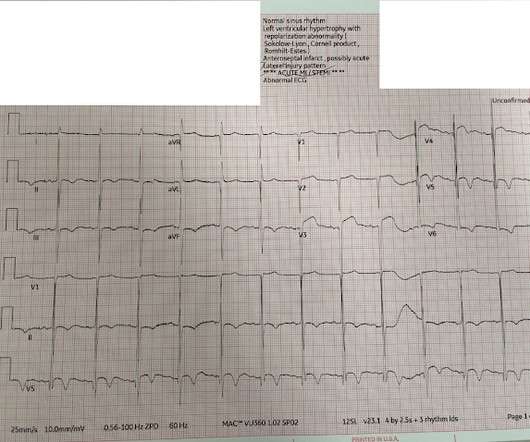
Written by Jesse McLaren Four patients presented with chestpain. If you were working in a busy emergency department, would you like to be interrupted to interpret these ECGs or can these patients safely wait to be seen because of the normal computer interpretation?
Jesse McLaren (@ECGcases), of Emergency Medicine Cases Reviewed by Pendell Meyers and Steve Smith An 85yo with a history of hypertension developed chestpain and collapsed, and had bystander CPR. The paramedics found the patient with ROSC and a GCS 7, and an ECG showing LBBB with possible lateral ST elevation. Learning points 1.
The above is what I thought when I saw this, so I went to the chart and found this history: A type I diabetic aged approximately 35 years old presented with chestpain, nausea, vomiting and diffuse abdominal pain. The patient was in DKA with an anion gap of 35, a glucose of 1128, and a K of 5.5 It was stented.
24 and how those may impact clinical practice and patientcare in this deep dive clinical trial session. ET Murphy Ballroom 4 ACC.24 24 planners note that attendees can gain insights from key clinical trials presented at ACC.24 More information: www.acc.org If you enjoy this content, please share it with a colleague
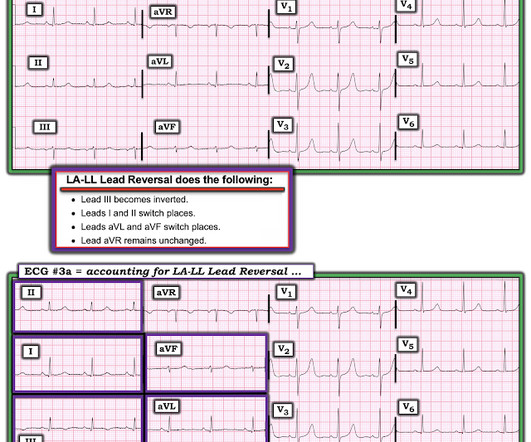
Even if you don't see the OMI, you can usually prevent such a long delay to reperfusion by recording serial ECGs every 15 minutes for a patient with persistent chestpain. Record serial ECGs every 15 minutes!! Hillinger et al. If not — Do you think this would be helpful? The rhythm in ECG #1 is sinus bradycardia and arrhythmia.
Written by Pendell Meyers, few edits by Smith A man in his 60s with history of stroke and hypertension but no known heart disease presented with chestpain that started on the morning of presentation at around 8am. Here is his triage ECG when he presented at 1657: What do you think? There, one sees typical STEMI to one's satisfaction.
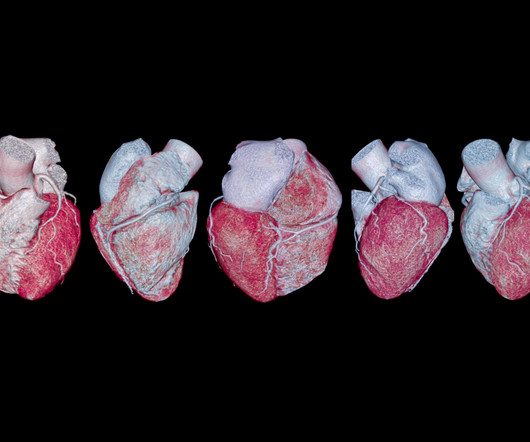
Cardiac CT scans, recommended by the American College of Cardiology (ACC) and the American Heart Association (AHA) as the primary testing strategy for patients with acute chestpain, are necessary for evaluating cases and determining treatment plans. As a result, we can provide more proactive patientcare.
Their teamwork and collaboration, allows us to advance collective efforts within this sector, driving forward innovation and enhancing patientcare," said SCAI Interventional Cardiology Program Chair, J. About 276,000 patients have undergone a TAVR procedure in the United States.
The recent change in guidelines from the ACC and AHA are now clear that cardiac CT is the Level 1A evidence recommended test for diagnosis of stable and acute chestpain,” said Chaim Lotan, MD, professor at Hadassah-Hebrew University, in a written statement from Arineta. Education and training.
Early Signs of Cardiac Trouble in Women Recognizing the early signs of cardiac trouble in women, such as chestpain, shortness of breath, unexplained fatigue, jaw pain, nausea, and lightheadedness, is crucial for prompt medical intervention and improved long-term outcomes.
The patient advised overall improvement with complete resolution of symptoms. The patientcare narrative states no further changes in heart rate with persistent LBBB morphology. Hospital transport was unremarkable. He received a permanent pacemaker during the subsequent inpatient stay.
Written by Hans Helseth A 34 year old man with no known medical history presented to the ED after an hour of chestpain. He described the pain as a mid sternal "burning sensation" and rated it 8.5 out of 10 at onset, but on presentation to the ED, reported that the pain had improved to 4.5. Patient has 4.5/10
Fortunately, the physicians seeing the patient were using the Queen of Hearts PM Cardio AI ECG OMI Model, and she had absolutely no concerns. When the Queen has some suspicion of OMI, she asks if the patient has ACS Symptoms. When I reviewed the chart, I learned that the patient had presented with syncope.
Check : [vitals, SOB, ChestPain, Ultrasound] If the patient has Abdominal Pain, ChestPain, Dyspnea or Hypoxemia, Headache, Hypotension , then these should be considered the primary chief complaint (not syncope). Outcomes in Presyncope Patients: A Prospective Cohort Study.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



















Let's personalize your content