This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The patient presented to an outside hospital An 80yo female per triage “patient presents with chestpain, also hurts to breathe” PMH: CAD, s/p stent placement, CHF, atrial fibrillation, pacemaker (placed 1 month earlier), LBBB. HPI: Abrupt onset of substernal chestpain associated with nausea/vomiting 30 min PTA.
No ChestPain, but somnolent. The fact that this is syncope makes give it a far lower pretest probability than chestpain, but it was really more than syncope, as the patient actually underwent CPR and had hypotension on arrival of EMS. Smith : "What was the outcome?" They of course opened and stented it.
A 50-something male with hypertension and 20- to 40-year smoking history presented with 1 week of stuttering chestpain that is worse with exertion, which takes many minutes to resolve after resting and never occurs at rest. At times the pain does go to his left neck. It is a ssociated with mild dyspnea on exertion.
Written by Magnus Nossen with Edits by Grauer and Smith The ECGs in today’s case are from 3 different patients all presenting with new-onset CP ( ChestPain ). As a result, this 45-year old man did not experince any delay in treatment — and a large diagonal branch of the LAD was stented with good outcome.
Written by Jesse McLaren, comments by Smith A 55 year old with a history of NSTEMI presented with two hours of exertional chestpain, with normal vitals. Old ‘NSTEMI’ A history of coronary artery disease and a stent to the same territory further increases pre-test likelihood of acute coronary occlusion, including in-stent thrombosis.
Written by Pendell Meyers A man in his early 40s experienced acute onset chestpain. The chestpain started about 24 hours ago, but there was no detailed information available about whether his pain had come and gone, or what prompted him to be evaluated 24 hours after onset.
A 40-something male presented by ambulance with one hour of chestpain that was improving after sublingual nitroglycerine and 325 mg of aspirin, chewed. It must have re-occluded between the ED and the cath lab) --Lesion was stented. Here is his initial ED ECG: What do you think?
A 50-something man presented in shock with severe chestpain. Angiogram: Culprit Lesion (s): Thrombotic occlusion of the proximal RCA -- stented. His prehospital ECG was diagnostic of inferior posterior OMI. The patient was in clinical shock with a lactate of 8. He appeared gray in color, with cool skin.
Submitted and written by Anonymous, edits by Meyers and Smith A 50s-year-old patient with no known cardiac history presented at 0045 with three hours of unrelenting central chestpain. The pain was heavy, radiated to her jaw with an associated headache. A single DES stent was placed, and the patient did well post-procedure.
Case submitted by Rachel Plate MD, written by Pendell Meyers A man in his 70s presented with chestpain which had started acutely at rest and has lasted for 2 hours. The pain was still ongoing at arrival. He also noted a bilateral "odd feeling" in his arms. He stated it was similar to prior heart attacks.
This case was texted to me by one of our residency graduates, and with the outcome, so I don't know how I would have interpreted it blindly. A 50-something male who is healthy and active with no previous medical history presented with 5 hours of continuous worrisome chestpain. It was opened and stented. is worrisome!
He had suffered a couple bouts of typical chestpain in the last 24 hours. This ECG (ECG #3) was recorded immediately after the last episode of pain spontaneously resolved. The pain had lasted about one hour. More outcome Peak troponin I was 0.58 Case A 40-something male presented to triage. Am J Cardiol.
A 60-something woman called EMS for chestpain. link] Clinical Course I don't know if the medics noticed these ECG findings or not, but if not, they recognized the value of serial ECGs in a patient with chestpain. The medics administered aspirin (no Nitroglycerine), and the pain resolved. #5: mm in V2 and 0.65
Written by Willy Frick A man in his 50s with a history of hypertension, dyslipidemia, type 2 diabetes mellitus, and prior inferior OMI status post DES to his proximal RCA 3 years prior presented to the emergency department at around 3 AM complaining of chestpain onset around 9 PM the evening prior. The following ECG was obtained.
A male in his 40's who had been discharged 6 hours prior after stenting of an inferoposterior STEMI had sudden severe SOB at home 2 hours prior to calling 911. He had no chestpain. Medications were aspirin, clopidogrel, metoprolol, and simvastatin. He was in acute distress from pulmonary edema, with a BP of 180/110, pulse 110.
After only 90 minutes of chestpain, the first troponin was unsurprisingly in the normal range at 11ng/L (normal <26 in males and <16 in females), so the emergency physician waited for repeat troponin. Chestpain still persists. Paged cardiology 0800: patient complains of chestpain. Cardiology aware.
No patient with chestpain should be sent home without troponin testing. All three lesions had TIMI 2 flow prior to stenting. This is an RAO cranial projection of the left coronary vessels after thrombectomy and stenting. The patient was sent home with a prescription for omeprazole to treat presumed peptic disease.
There is new data showing better outcomes when bystander lesions (non-culprit) are stented. == MY Comment by K EN G RAUER, MD ( 8/28/2020 ): == Dr. Smith highlights a number of important lessons to be learned from today’s case. Sotalol prolongs the QT 7. I limit my comments to some additional points of interest.
On the second morning of his admission, he developed 10/10 chestpain and some diaphoresis after breakfast. The patient was given opiates which improved his chestpain to 7/10. The consulting cardiologist wrote in their note: “Could be cardiac chestpain. She is usually incredibly good at recognizing them!
Sent by anonymous, written by Pendell Meyers Case 1: A man in his 50s presented with acute chestpain. The cath lab was activated, and then not cancelled, and the angiogram showed 99% TIMI 2 flow proximal LAD culprit lesion, stented in less than 90 minutes of arrival. Outcome of case 2? Normal vital signs. Normal vitals.
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chestpain similar to his prior MI, but worse. The pain initially started the day prior to presentation. mV compared to 0.05-0.1
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chestpain relieved by rest. This episode of chestpain began 3 hours ago and was persistent even at rest. Troponin was ordered.
There was no chestpain or SOB, at least none reported by Dr. Lee. Given that this patient has no chestpain, one must be skeptical of such a diagnosis. Outcome : She ruled in for MI by troponins and went for angiogram. An 80% thrombotic RCA was stented. This case was sent by Arthur Lee. This is not normal.
Written by Pendell Meyers Two adult patients in their 50s called EMS for acute chestpain that started within the last hour. Patient 2 Clinical Course and Outcome: This patients first ECG was sent to the EM physician who said it did not meet STEMI criteria, but wisely agreed with EMS to get serial ECGs during transport.
This was texted to me from a former resident, while working at a small rural hospital, with the statement: "I can’t convince myself of anything here, but he’s a 63-year-old guy with prior stents and a good story for ACS." Chestpain or discomfort) What do you think? The total duration of chestpain was 30-45 minutes.
This male in his 40's had been having intermittent chestpain for one week. He awoke from sleep with crushing central chestpain and called ems. EMS recorded a 12-lead, then gave 2 sublingual nitros with complete relief of pain. A stent was placed. Type B waves are deeper and symmetric.
Written by Pendell Meyers, edits by Smith: Case A 72 year old female with hypertension and COPD presented with sudden shortness of breath and chestpain. On day 3 of hospitalization she underwent coronary angiography, revealing a 95% lesion in the mid-LAD which was stented. There is sinus rhythm with PACs and PVCs.
This 42 yo diabetic male presented with cough and foot pain. In spite of aggressive questioning, he denied chestpain, but he did tell one triage nurse that he had had some chest burning, and so he underwent an ECG: There are deep Q-waves and QS-waves in precordial leads V2-V3, with a bit of R-wave left in V4.
This is the initial ED ECG of a 46 year old male with chestpain: The QTc was 420 ST Elevation at 60 ms after the J-point in lead V3 = 2.5 ng/ml) A 45 year old male called 911 for chestpain: The QTc was 400 ST Elevation at 60 ms after the J-point in lead V3 = 3.5 100% LAD occlusion. He underwent CABG. QRS V2 = 15.5
This was a male in his 50's with a history of hypertension and possible diabetes mellitus who presented to the emergency department with a history of squeezing chestpain, lasting 5 minutes at a time, with several episodes over the past couple of months. Plan was for admission for chestpain workup. It was stented.
Case A 47 year old male called 911 for severe chestpain. Jason asked me if I thought it is due to occlusion (without either of us knowing the outcome), and this was my answer: This is a posterolateral MI. It was opened and stented. Culprit, stented) 3. The patient had never had pain like this before.
In that case, the patient did not have chestpain but was 36 years old. This patient does not have chestpain but is elderly and that increases the pretest probability by a huge amount.
This fantastic case and post was written by Jesse McLaren (@ECGcases), edited by Smith Case You’re shown an ECG from a patient in the waiting room with chestpain. It was a 60yo with a history of stents to the circumflex and right coronary arteries, who presented with 9 hours of fluctuating central chestpain.
The lesion was stented. The 1st “lesson” is, “All bets are off” — when an adult of any age presents to the ED with new-onset chest discomfort. Although by the time you are reading My Comment, you already know the outcome in this case — GO BACK and Take Another Look at the initial ECG @ Time = 0:00 ( TOP tracing in Figure-1 ).
A 40 something otherwise healthy man presented with substernal chestpain. They were stented. Emergent cardiac outcomes in patients with normal electrocardiograms in the emergency department. It had occurred once 3 days prior and resolved without any medical visit. What do you think? The peak troponin was 1863 ng/L.
Stone, MD Mount Sinai Health System tim.hodson Wed, 04/02/2025 - 15:26 March 31, 2025 Using intravascular imaging (IVI) to guide stent implantation during complex stenting procedures is safer and more effective for patients with severely calcified coronary artery disease than conventional angiography, the more commonly used technique.
This was sent by anonymous The patient is a 55-year-old male who presented to the emergency department after approximately 3 to 4 days of intermittent central boring chestpain initially responsive to nitroglycerin, but is now more constant and not responsive to nitroglycerin. It is unknown when this pain recurred and became constant.
Given the presentation, the cardiologist stented the vessel and the patient returned to the ICU for ongoing critical care. He did not remember whether he had experienced any chestpain. (TIMI 3 means the rate of passage of dye through the coronary artery is normal by angiography.) Two subsequent troponins were down trending.
Delayed angiogram found a 95% mid RCA occlusion that was stented. 1] The patient did not have a good outcome because their ECG was labeled ‘normal’ but in spite of it. Smith : this proves my impression that the inferior T-waves on the first ECG are hyperacute.
TheNational Institute for Health and Care Excellence(NICE) recommends CCTA as the first-line investigation for patients with chestpain due to suspected CAD, highlighting its importance in improving diagnostic certainty. viii, ix, x, xi, xii, xiii, xiv, xv GE HealthCaredesigned Revolution Vibe to address these challenges.
A male in late middle age with a history of RCA stent 8 years prior complained of chestpain. It is highly associated with proximal LAD occlusion and bad outcomes. EMS recorded the following ECG: What do you see? I have annotated it here: The lines mark the end of the QRS and beginning of the ST segment.
See this case: Persistent ChestPain, an Elevated Troponin, and a Normal ECG. This is different from nitroglycerin which produces vasodilation and can improve by pain improving myocardial perfusion. Here is the angiogram after stent placement. link] Opiates are associated with worse outcomes in Myocardial Infarction.
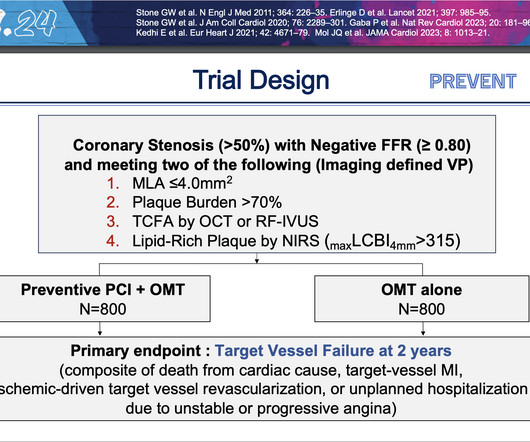
At two years, people who underwent preventive PCI were 89% less likely to experience the composite primary endpoint of cardiac death, heart attack in the target vessel, revascularization due to ischemia in the target vessel or hospitalization for unstable or progressive chestpain compared with people who received medications alone.
The impact of this narrowing can ultimately result in angina (chestpain), which has been shown to double the risk of major cardiovascular events,1 as well as myocardial infarction ( heart attack ) or even death. Accessed May 2024. Kirtane, Yongjian Wu, William Wijns, Weixian Yang, Martin B. Leon, Shubin Qiao, Gregg W.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.














































Let's personalize your content