This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A 50-something male had onset of chestpain 1 hour prior to ED arrival. Endorses some associated SOB, but denies back pain, fever, cough, chills, leg swelling, or other new symptoms. It was tested on a large database of known outcomes and was more than twice as senstivity as STEMI criteria and much better than cardiologists.
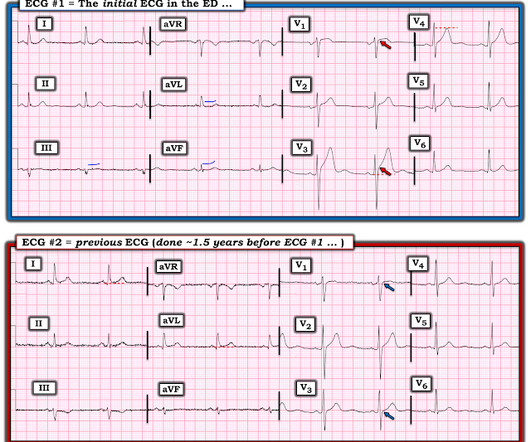
A 50-something male with hypertension and 20- to 40-year smoking history presented with 1 week of stuttering chestpain that is worse with exertion, which takes many minutes to resolve after resting and never occurs at rest. At times the pain does go to his left neck. It is a ssociated with mild dyspnea on exertion.
The patient presented to an outside hospital An 80yo female per triage “patient presents with chestpain, also hurts to breathe” PMH: CAD, s/p stent placement, CHF, atrial fibrillation, pacemaker (placed 1 month earlier), LBBB. HPI: Abrupt onset of substernal chestpain associated with nausea/vomiting 30 min PTA.
Written by Jesse McLaren, comments by Smith A 55 year old with a history of NSTEMI presented with two hours of exertional chestpain, with normal vitals. See these posts: ChestPain, ST Elevation, and an Elevated Troponin: Should we Activate the Cath Lab? What do you think?
A 40-something male presented by ambulance with one hour of chestpain that was improving after sublingual nitroglycerine and 325 mg of aspirin, chewed. Here is the angiogram: --Culprit is 100% stenosis in the proximal RCA. (It Here is his initial ED ECG: What do you think? Then the ED doc would be dependent on that first ECG.
Sent by anonymous, written by Pendell Meyers A man in his 50s with no prior known medical history presented to the Emergency Department with severe intermittent chestpain. He denied any lightheadedness, shortness of breath, vomiting, or abdominal pain. Isn't it amazing?? hours earlier? Circulation. 2001;104:636–641.
Submitted and written by Megan Lieb, DO with edits by Bracey, Smith, Meyers, and Grauer A 50-ish year old man with ICD presented to the emergency department with substernal chestpain for 3 hours prior to arrival. At this time he reported ongoing chestpain and was given aspirin and nitroglycerin.
There is a patient with persistent chestpain and an initial troponin I over 52 ng/L; 52 ng/L has an approximate 70% PPV for acute type I MI in a chestpain patient. Pain was severe and persistent. CT angiography chest assessing for PE and dissection negative. Heparin drip was initiated. Normal RV function.
He had suffered a couple bouts of typical chestpain in the last 24 hours. This ECG (ECG #3) was recorded immediately after the last episode of pain spontaneously resolved. The pain had lasted about one hour. More outcome Peak troponin I was 0.58 Case A 40-something male presented to triage. Am Heart J.
This study investigated the clinical characteristics and clinical outcomes in patients with VSA and OCAD, especially regarding provoked spasm phenotypes and sites. We defined positive epicardial spasm as ≥90% transient stenosis and usual chest symptoms or ischemic ECG changes.
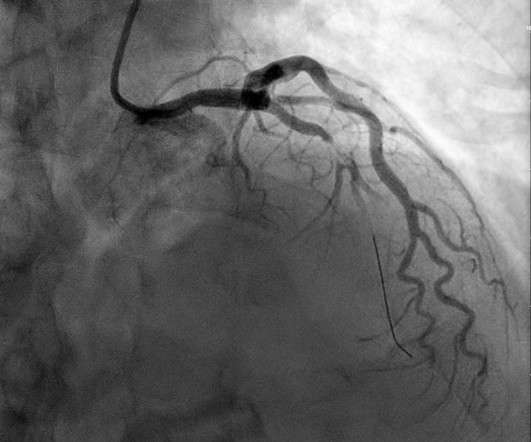
No patient with chestpain should be sent home without troponin testing. The red arrow shows a roughly 80% stenosis of the proximal LAD. The blue arrow shows another stenosis of the LAD distal to the first diagonal branch of about 99%. The green arrow shows a 95% stenosis of the ostium of the first diagonal branch.
A 20-something male presented from an outside facility with Chestpain. He came with this ECG from the outside facility, recorded 1 hour after pain onset: There is at least 2 mm of inferior ST elevation, with reciprocal ST depression in aVL, ST flattening in V4-V6, and T-wave inversion in V2. Vital signs were normal.
Here I annotate it: This shows 100% occluded circumflex (red arrow) and a 90% stenosis of the LAD (Yellow arrow). The LAD was thought to be not thrombotic, but a chronic tight stenosis. My THOUGHTS on ECG #1: We are told that the patient in today’s case had an episode of severe chestpain 3 nights prior to admission.
On the second morning of his admission, he developed 10/10 chestpain and some diaphoresis after breakfast. The patient was given opiates which improved his chestpain to 7/10. The consulting cardiologist wrote in their note: “Could be cardiac chestpain. She is usually incredibly good at recognizing them!
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chestpain similar to his prior MI, but worse. The pain initially started the day prior to presentation. The ST elevation from today is ~0.2
A 70-something female with no previous cardiac history presented with acute chestpain. She awoke from sleep last night around 4:45 AM (3 hours prior to arrival) with pain that originated in her mid back. She stated the pain was achy/crampy. Over the course of the next hour, this pain turned into a pressure in her chest.
This male in his 40's had been having intermittent chestpain for one week. He awoke from sleep with crushing central chestpain and called ems. EMS recorded a 12-lead, then gave 2 sublingual nitros with complete relief of pain. Type B waves are deeper and symmetric. Wellen's syndrome is a Reperfusion syndrome.
This year’s theme, “Advancing Cardiovascular Care for All” brings the latest practice-changing breakthroughs, along with top experts debating and discussing outcomes of highly-anticipated clinical trials. 24 from April 6 - 8, 2024 in Atlanta, GA at the Georgia World Congress Center.
COPD, Idiopathic PAH, acute or chronic PE, pulmonary valve stenosis, etc) 3) Conditions affecting RV myocardial contractility, such as ARVD or RV infarction The ECGs does not really show any signs of chronic RV dilation or hypertrophy. Any cause of pulmonary hypertension. Our THANKS to Dr. Magnus Nossen for sharing this case with us.
This patient, who is a mid 60s female with a history of hypertension, hyperlipidemia and GERD, called 911 because of chestpain. A mid 60s woman with history of hypertension, hyperlipidemia, and GERD called 911 for chestpain. It is also NOT the clinical scenario of takotsubo (a week of intermittent chestpain).
This is the initial ED ECG of a 46 year old male with chestpain: The QTc was 420 ST Elevation at 60 ms after the J-point in lead V3 = 2.5 ng/ml) A 45 year old male called 911 for chestpain: The QTc was 400 ST Elevation at 60 ms after the J-point in lead V3 = 3.5 Angiogram showed a critical LAD thrombotic stenosis.
Full case details and outcomes are below. The Queen of Hearts correctly says: Smith : Why is this ECG which manifests so much ST Elevation NOT a STEMI (even if it were a 60 year old with chestpain)? Repeat 0157 with ongoing chestpain: Basically the same features diagnostic of LAD occlusion. Physician: "No STEMI."
Case A 47 year old male called 911 for severe chestpain. Jason asked me if I thought it is due to occlusion (without either of us knowing the outcome), and this was my answer: This is a posterolateral MI. LM: No significant stenosis. LAD: luminal irregularities with a 40% stenosis at the take-off of a D3.
Written by Pendell Meyers, edits by Smith Two patients presented with acute chestpain/pressure. There is no mention of whether the patient had any pain at this time. Cath was done at around 9AM: Culprit lesion mid-LAD, 99% stenosis, pre-intervention TIMI flow not listed, PCI performed with TIMI 3 flow and 0% stenosis resulting.
The best course is to wait until the anatomy is defined by angio, then if proceeding to PCI, add Cangrelor (an IV P2Y12 inhibitor) I sent the ECG and clinical information of a 90-year old with chestpain to Dr. McLaren. 2 cases of Aortic Stenosis: Diffuse Subendocardial Ischemia on the ECG. Anything more on history? Left main?
We knew only that the ECG belonged to a man in his 50s with chestpain and normal vitals. The day prior to presentation (about 12 hours prior to presentation) he described sudden onset chestpain and shortness of breath while gardening in his back yard. He had no further pain and went to bed that night with no complaints.
Sent by anonymous, edited by Pendell Meyers A man in his 50s with history only of hypertension presented with acute chestpain that started 45 minutes prior to presentation while doing yard work. The culprit lesion was a complex calcified mid LAD stenosis involving the first and second diagonal branches. Am Heart J.
Written by Pendell Meyers A man in his 40s called EMS for acute chestpain that awoke him from sleep, along with nausea and shortness of breath. Long term outcome is unavailable. His history included known heart failure with prior EF 18%, insulin dependent diabetes, and polysubstance abuse.
Early detection through regular heart check-ups, including listening for murmurs, can lead to timely treatment and improved outcomes. The earlier we catch it, the more treatment options we have, and the better the outcome for the patient. Many people with HVD may not experience symptoms until the disease reaches an advanced stage.
Objectives Patients presenting with suspected ST segment elevation myocardial infarction frequently have symptoms in addition to chestpain, including dyspnea, nausea or vomiting, diaphoresis, and lightheadedness or syncope. These symptoms are often regarded as supporting the diagnosis of infarction.
Edits by Meyers and Smith A man in his 70s with PMH of hypertension, hyperlipidemia, type 2 diabetes, CVA, dual-chamber Medtronic pacemaker, presented to the ED for evaluation of acute chestpain. So the patient was taken for emergent cath, showing: Culprit artery: LAD (100% stenosis, TIMI 0) requiring thrombectomy and stent.
ChestPain – Benign Early Repol or OMI? Written by Destiny Folk, MD, Adam Engberg, MD, and Vitaliy Belyshev MD A man in his early 60s with a past medical history of hypertension, type 2 diabetes, obesity, and hyperlipidemia presented to the emergency department for evaluation of chestpain.
We believe the tools, resources, and information shared at the meeting will provide the healthcare community with greater expertise to improve patient outcomes and also connect with their interventional cardiology colleagues,” said SCAI President George D. Dangas, MD, PhD, MSCAI , Icahn School of Medicine - Mt.
Written by Pendell Meyers Both of these cases were sent to me with no information other than adults with acute chestpain. Case 1 An elderly male presented with chestpain. Case 2 A man in his 60s presented with acute chestpain, about 1 hour prior to evaluation: What do you think? We will study this soon.
Soviet biologist Trofim Lysenko famously rejected the objective reality of Mendelian genetics because it clashed with the Marxist philosophy that the environment, not genetics, was the primary determinant of outcomes. Atypical angina is classified as having any two of the three symptoms, and non-anginal pain any one of the three symptoms.
He was at the gym when he had the onset of chestpain. Angiography revealed a very tight LAD stenosis with some flow (confirming the reperfusion that we see on the ECG). A stent was placed, and the patient had an excellent outcome with no wall motion abnormality. This patient is 38 years old with hyperlipidemia.
A reliable study would keep track of all patients with shockable arrest and analyze the ones who were not enrolled to see their outcomes. This is a primary ST-T wave change , that in a patient with chestpain ( or cardiac arrest ) — indicates an ongoing acute event until proven otherwise. This study failed to do so.
When we observed that bicuspid aortic valve is kind of a risk marker for this group with bad outcomes, we specifically wanted to see whether young individuals who present clinically due to problems related to bicuspid aortic valve disease may also have rare genetic variants that predict complications such as needing valve surgery.”
Case 3 : Male in 30's with chestpain, cough, and fever. Is there likely to be fixed coronary stenosis that led to demand ischemia during pneumonia? --Was A male in late middle age with a history of RCA stent 8 years prior complained of chestpain. What do you think? He has clinical pneumonia. Called 911.
This distinction is crucial to understand as most heart attacks result from plaque ruptures of less than 70% stenosis, which is the type of narrowing missed by most exercise stress tests 2. Estimates of Angiographic Stenosis of Culprit Coronary Artery Lesions in 50 Consecutive Patients Experiencing Sudden Coronary Death.
His comments/questions are inserted below the ECG: A 50-something woman presented with 3 days of intermittent chestpain that became worse on the day of presentation, with diaphoresis and radiation to the left arm, as well as abdominal pain. TIMI 0/1 flow).(61,62) Knotts et al. Zoghbi GJ, Misra VK, Brott BC, et al.
Aortic Dissection, Valvular (especially Aortic Stenosis), Tamponade. Check : [vitals, SOB, ChestPain, Ultrasound] If the patient has Abdominal Pain, ChestPain, Dyspnea or Hypoxemia, Headache, Hypotension , then these should be considered the primary chief complaint (not syncope). orthostatic vitals b.
A 69 year old woman with a history of hypertension presented to the emergency department by EMS for evaluation of chestpain and shortness of breath. She awoke in the morning with sharp chestpain which worsened throughout the morning. As her pain worsened, so did her dyspnea. This was written by Hans Helseth.
Written by Pendell Meyers, few edits by Smith A woman in her 70s was woken from sleep by midsternal chestpain radiating to left arm with nausea. The history in today's case is classic for an acute cardiac event — as this older woman was awakened from sleep by chestpain radiating to her left arm with nausea.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.















































Let's personalize your content