This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
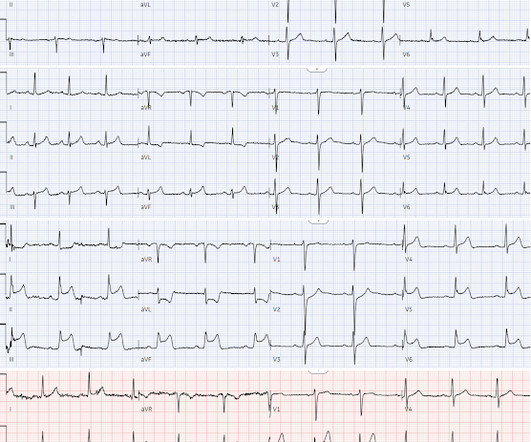
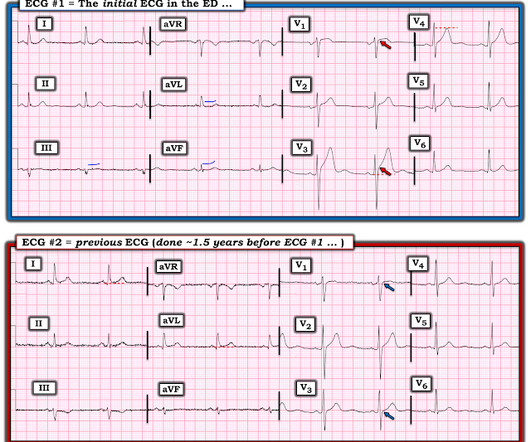
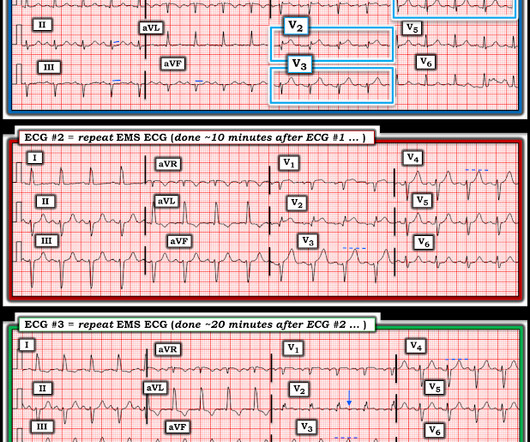
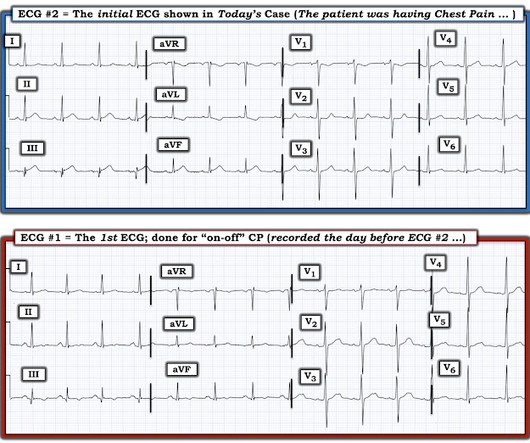
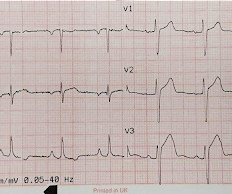
2 middle aged males presented with chestpain. Which had the more severe chestpain at the time of the ECG? Patient 2 at the bottom with a very subtle OMI complained of 10/10 chestpain at the time the ECG was recorded. 414 patients were included in the analysis.
Written by Jesse McLaren A 45-year-old presented with 24 hours of intermittent chestpain. On it’s own this is nonspecific, but in the right context this could be diagonal occlusion (if active chestpain) or infero-posterior reperfusion (if resolved chestpain). #2 What was the outcome and final diagnosis?
Written by Pendell Meyers A man in his 40s called EMS for acute chestpain that awoke him from sleep, along with nausea and shortness of breath. Long term outcome is unavailable. There is no recognition of STEMI equivalency in this setting in the USA guidelines currently. So the cath lab was activated.
This was sent by anonymous The patient is a 55-year-old male who presented to the emergency department after approximately 3 to 4 days of intermittent central boring chestpain initially responsive to nitroglycerin, but is now more constant and not responsive to nitroglycerin. It is unknown when this pain recurred and became constant.
Written by Jesse McLaren A 50 year old presented to triage with one hour of chestpain, and the following ECG labeled normal by the computer (GE Marquette SL) algorithm. They concluded, "Our findings increase confidence in the normal automated GE Marquette 12 SL ECG software interpretation to predict a benign outcome.
A 50-something male had onset of chestpain 1 hour prior to ED arrival. Endorses some associated SOB, but denies back pain, fever, cough, chills, leg swelling, or other new symptoms. It was tested on a large database of known outcomes and was more than twice as senstivity as STEMI criteria and much better than cardiologists.
Written by Jesse McLaren A 65 year old with a history of atrial flutter, CABG and end-stage renal disease on dialysis presented with 3 days of fluctuating chestpain, which was ongoing at triage. So a patient with high pretest probability (prior CABG with new chestpain), had new ECG changes showing posterior OMI.
Sent by Magnus Nossen MD, written by Pendell Meyers A man in his 50s, previously healthy, developed acute chestpain. The primary care physician there evaluated this patient and deemed the chestpain to be due to gastrointestinal causes. link] ] Outcome The patient emerged neurologically intact.
Written by Colin Jenkins and Nhu-Nguyen Le with edits by Willy Frick and by Smith A 46-year-old male presented to the emergency department with 2 days of heavy substernal chestpain and nausea. The patient continued having chestpain. Is there STEMI? Fortunately the patient was then taken for angiography.
Written by Jesse McLaren Four patients presented with chestpain. 1-3] But these studies were very short duration and used cardiology interpretation of ECGs or emergent angiography rather than patient outcomes. have published a number of warnings about the previous reassuring studies.[4,5] minutes).
This was sent by Sam Ghali @EM_RESUS A 44 year old man presented with chestpain The tech came running with the ECG as the computer called "STEMI!" Tell me the outcome! So signed it NO STEMI and triaged him OK to not be in RESUS." What do you think? Sam sent this to me and asked: "What do you think, Steve?"
Written by Jesse McLaren A previously healthy 60 year old developed exertional chestpain with diaphoresis, and called EMS. So while there’s no diagnostic STEMI criteria, there are multiple ischemic abnormalities in 11/12 leads involving QRS, ST and T waves, which are diagnostic of a proximal LAD occlusion. What do you think?
A 50-something male with hypertension and 20- to 40-year smoking history presented with 1 week of stuttering chestpain that is worse with exertion, which takes many minutes to resolve after resting and never occurs at rest. At times the pain does go to his left neck. What do you think the prehospital ECG showed (with pain)?
Written by Jesse McLaren, comments by Smith A 55 year old with a history of NSTEMI presented with two hours of exertional chestpain, with normal vitals. See these posts: ChestPain, ST Elevation, and an Elevated Troponin: Should we Activate the Cath Lab? So this NSTEMI was likely a STEMI(-)OMI with delayed reperfusion.
Written by Jesse McLaren Three patients presented with acute chestpain and ECGs that were labeled by the computer as completely normal, and which was confirmed by the final cardiology interpretation (which is blinded to patient outcome) also as completely normal. What do you think?
The patient presented to an outside hospital An 80yo female per triage “patient presents with chestpain, also hurts to breathe” PMH: CAD, s/p stent placement, CHF, atrial fibrillation, pacemaker (placed 1 month earlier), LBBB. HPI: Abrupt onset of substernal chestpain associated with nausea/vomiting 30 min PTA.
Click here to sign up for Queen of Hearts Access Case A 58-year-old woman presented to the ED with burning chestpain that started 2-3 hours earlier while sitting on a porch swing. See this post: Septal STEMI with ST elevation in V1 and V4R, and reciprocal ST depression in V5, V6. Also seen in inferior + RV OMI.)
Written by Magnus Nossen with Edits by Grauer and Smith The ECGs in today’s case are from 3 different patients all presenting with new-onset CP ( ChestPain ). It definitely does not fulfill STEMI criteria, and I would argue that it would not lead to cath lab activation in most centers. The ECG shows ST depression in lead V3.
Written by Pendell Meyers A man in his early 40s experienced acute onset chestpain. The chestpain started about 24 hours ago, but there was no detailed information available about whether his pain had come and gone, or what prompted him to be evaluated 24 hours after onset. And yet it still says "normal".
A 40-something male presented by ambulance with one hour of chestpain that was improving after sublingual nitroglycerine and 325 mg of aspirin, chewed. Here it is: Obvious Inferior Posterior STEMI (+) OMI. Initial troponin was: 3 ng/L We showed that the first troponin in acute STEMI is often negative in at least 27%.
A 67 yo f developed chestpain this morning." Cath lab declined as it is not a STEMI." And now this finding is even formally endorsed as a "STEMI equivalent" in the 2022 ACC guidelines!!! Another myocardial wall is sacrificed at the altar of the STEMI/NonSTEMI mindset. See this case: A man his 50s with chestpain.
Written by Pendell Meyers A woman in her 70s had acute chestpain and called EMS. Interpretation : diagnostic of acute anterior OMI with STE less than STEMI criteria in V1-V4, hyperacute T waves in V2-V4, and suspiciously flat isoelectric ST segments in III and aVF suspicious for reciprocal findings. Ongoing OMI.
Submitted by Dr. Dennis Cho (@DennisCho), written by Jesse McLaren A 70-year-old with no cardiac history presented with 2 hours of chestpain radiating to the neck, associated with shortness of breath. Fortunately, Dr. Cho was not looking for STEMI ECG criteria but for an acute coronary occlusion. OMI or STEMI?
A healthy 45-year-old female presented with chestpain, with normal vitals. The patient was previously healthy, with no atherosclerotic risk factors, and developed chestpain after an episode of stress. The pain was crushing retrosternal, radiated to the arms and was associated with lightheadedness.
A 29 year old male presented with 6 hours of stuttering chestpain, constant for the last hour, worse with breathing. Diagnosis: There are Q-waves, ST elevation, and hyperacute T-waves in V2 and V3, diagnostic of acute LAD occlusion (STEMI). Take home point here : Obtain an ECG on anyone with chestpain.
Sent by anonymous, written by Pendell Meyers A man in his 50s with no prior known medical history presented to the Emergency Department with severe intermittent chestpain. He denied any lightheadedness, shortness of breath, vomiting, or abdominal pain. Barely any STE, and thus not meeting STEMI criteria.
A 50-something man presented in shock with severe chestpain. There is an obvious inferior posterior STEMI(+) OMI. Methods Retrospective study of consecutive inferior STEMI , comparing ECGs of patients with, to those without, RVMI, as determined by angiographic coronary occlusion proximal to the RV marginal branch.
Theres ST elevation in V3-4 which meets STEMI criteria, which could be present in either early repolarization, pericarditis or injury. Lets see what happens in the current STEMI paradigm. Emergency physician: STEMI neg but with elevated troponin = Non-STEMI The first ECG was signed off. Chestpain still persists.
There were no injuries and no chestpain and he appeared well. He complained of 3 days of diarrhea and abdominal pain. Jason was very skeptical of STEMI. This also argues against STEMI. What was the outcome? Look for old ECGs Do serial ECGs Do echocardiography June 17, 2016 Anterior STEMI?
A male in late middle age with a history of RCA stent 8 years prior complained of chestpain. It is highly associated with proximal LAD occlusion and bad outcomes. Here are three more dramatic cases that illustrate RBBB + LAFB Case 1 of cardiac arrest with unrecognized STEMI, died. New RBBB + LAFB is a very bad sign.
Written by Jesse McLaren, with comments from Smith A 50-year old patient on the medical wards developed acute chestpain, with an ECG labeled (see computer interpretation at the top) and confirmed as normal. In the STEMI paradigm, patients with ischemic symptoms and ECGs that don’t meet STEMI criteria get serial ECGs.
This is diagnostic of infero-posterior OMI, but it is falsely negative by STEMI criteria and with falsely negative posterior leads (though they do show mild ST elevation in V4R). Because the patient had no chestpain or shortness of breath, they were initially diagnosed as gastroenteritis. Potassium was normal. Take home 1.
Written by Pendell Meyers Both of these cases were sent to me with no information other than adults with acute chestpain. Case 1 An elderly male presented with chestpain. Case 2 A man in his 60s presented with acute chestpain, about 1 hour prior to evaluation: What do you think? We will study this soon.
A 70-year-old man calls 911 after experiencing sudden, severe chestpain. The precordial ST-depression pattern on this ECG (and in this clinical setting) should immediately raise suspicion of Posterior STEMI! But if there is none - then you are looking at least at an Isolated Posterior STEMI until proven otherwise.
[link] A 30 year-old woman was brought to the ED with chestpain. She had given birth a week ago, and she had similar chestpain during her labor. She attributed the chestpain to anxiety and stress, saying "I'm just an anxious person." examined SCAD presenting as STEMI (unlike Hassan et al.
Case 1: The outcome of this case is at the far bottom. He complained of severe chestpain and was extremely agitated, so much so that he was throwing chairs in triage. Technically, the STE meets STEMI criteria because there is greater than 2.5 These kinds of cases were excluded from the study as obvious anterior STEMI.
Submitted and written by Anonymous, edits by Meyers and Smith A 50s-year-old patient with no known cardiac history presented at 0045 with three hours of unrelenting central chestpain. The pain was heavy, radiated to her jaw with an associated headache. Triage VS: 135/65 mmHg, 95 bpm, 94% on room air, 16/min, 98.6 Lupu L, et al.
No prior exertional complaints of chestpain, dizziness, lightheadedness, or undue shortness of breath. He denied headache or neck pain associated with exertion. 50% of LAD STEMIs do not have reciprocal findings in inferior leads, and many LAD OMIs instead have STE and/or HATWs in inferior leads instead. Pericarditis?
A 61 year-old with chestpain arrived to the ED by ambulance with resolving chestpain. The chestpain is resolving, so if these are resolving hyperacute T-waves, then followup ECGs should show their size diminishing. The cath lab was activated, as it should be with transient STEMI. Learning Points 1.
There is clearly sufficient STE for STEMI criteria in leads V2 and aVL, but lead I has less than 1.0 mm of STE - thus, technically this ECG does not meet STEMI criteria, although it is a quite obvious OMI. This ECG was immediatel y discussed with the on-call cardiologist who said the ECG was "concerning but not a STEMI."
Case submitted by Rachel Plate MD, written by Pendell Meyers A man in his 70s presented with chestpain which had started acutely at rest and has lasted for 2 hours. The pain was still ongoing at arrival. He also noted a bilateral "odd feeling" in his arms. He stated it was similar to prior heart attacks.
Sent by Dan Singer MD, written by Meyers, edits by Smith A man in his late 30s presented with acute chestpain and normal vitals except tachycardia at about 115 bpm. Dr. Singer sent this to me with just the information: "~40 year old with acute chestpain". Other outcome information is not available.
There were no injuries and no chestpain and he appeared well. He complained of 3 days of diarrhea and abdominal pain. Jason was very skeptical of STEMI. This also argues against STEMI. What was the outcome? There was no chestpain. What do you think? Jason, I agree. Check for old records.
Submitted and written by Megan Lieb, DO with edits by Bracey, Smith, Meyers, and Grauer A 50-ish year old man with ICD presented to the emergency department with substernal chestpain for 3 hours prior to arrival. At this time he reported ongoing chestpain and was given aspirin and nitroglycerin.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






































Let's personalize your content