This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Acute pericarditis (AP) is the second most common cardiac cause of chestpain, diagnosed when at least two of the following criteria are met: characteristic pleuritic chestpain, pericardial rub on auscultation, new typical ECG changes (such as widespread ST-elevation or PR-depression) and pericardial effusion on imaging.
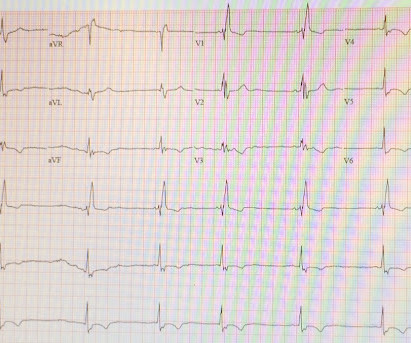
A healthy 45-year-old female presented with chestpain, with normal vitals. The computer interpretation was “ST elevation, consider early repolarization, pericarditis or injury.” The final cardiology interpretation confirmed the computer interpretation of “ST elevation, consider early repolarization, pericarditis or injury”.
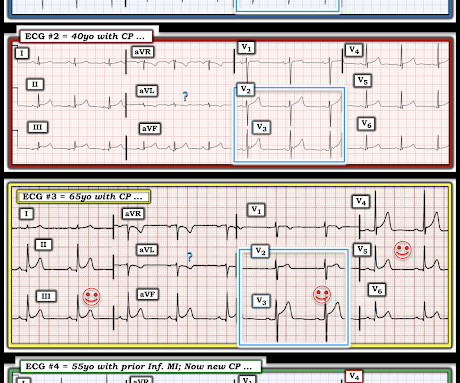
Written by Magnus Nossen with Edits by Grauer and Smith The ECGs in today’s case are from 3 different patients all presenting with new-onset CP ( ChestPain ). These latter findings are typical of pericarditis, but pericarditis never has reciprocal ST depression. This is OMI until proven otherwise.
Background There are limited data on acute pericarditis according to different age groups. The aim of this study is to investigate the role of age-related features in clinical characteristics, management, and outcomes of acute pericarditis, with a focus on the geriatric population. IQR 33–73) years, 32.3%
Sent by Dan Singer MD, written by Meyers, edits by Smith A man in his late 30s presented with acute chestpain and normal vitals except tachycardia at about 115 bpm. Dr. Singer sent this to me with just the information: "~40 year old with acute chestpain". Other outcome information is not available. Positional?
A 40 something woman with a history of hyperlipidemia and additional risk factors including a smoking history presented with substernal chestpain radiating to "both axilla" as well as the upper back. She was reportedly "pacing in her room while holding her chest". Clinician and EKG machine read of acute pericarditis.
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chestpain similar to his prior MI, but worse. The pain initially started the day prior to presentation. The ST elevation from today is ~0.2
Below is the first ECG, signed off by the over-reading cardiologist agreeing with the computer interpretation: ST elevation, consider early repolarization, pericarditis, or injury. Theres ST elevation in V3-4 which meets STEMI criteria, which could be present in either early repolarization, pericarditis or injury. What do you think?
Written by Pendell Meyers Two adult patients in their 50s called EMS for acute chestpain that started within the last hour. Of course the patient was saddled with the erroneous "pericarditis" diagnosis after CTs ruled also ruled out PE and dissection. Both were awake and alert with normal vital signs. What do you think?
Written by Pendell Meyers, edits by Smith: Case A 72 year old female with hypertension and COPD presented with sudden shortness of breath and chestpain. Peak troponin, echocardiographic findings, and long term outcome are unknown. There is sinus rhythm with PACs and PVCs. Learning Points: 1.
ECG of pneumopericardium and probable myocardial contusion shows typical pericarditis Male in 30's, 2 days after Motor Vehicle Collsion, complains of ChestPain and Dyspnea Head On Motor Vehicle Collision. RBBB in blunt chest trauma seems to be indicative of several RV injury. ST depression. Myocardial Contusion?
Written by Pendell Meyers, edits by Smith Two patients presented with acute chestpain/pressure. Two patients with chestpain. Learning Points It takes dedicated learning and observation of outcomes and serial ECGs to learn how to distinguish subtle OMI patterns from OMI mimics like the cases above.
For example, considering whatever symptoms that the patient may have had ( ie, chestpain, palpitations, shortness of breath, etc. ) — what this might mean in view of the ECG we are looking at. To quote Dr. Stephen Smith: "The worst risk factor for a bad outcome in acute MI is young age." Figure-2: I've labeled t he initial ECG.
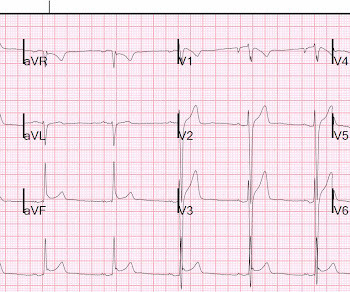
Written by Jesse McLaren Two patients presented with acute chestpain, and below are the precordial leads V1-6 for each. The initial computer and final cardiology interpretation was a differential: “ST elevation, consider early repolarization, pericarditis, or injury.” Are there 1 or 2 Leads that give you the answer?
Recall from this post referencing this study that "reciprocal STD in aVL is highly sensitive for inferior OMI (far better than STEMI criteria) and excludes pericarditis, but is not specific for OMI." See this case: Persistent ChestPain, an Elevated Troponin, and a Normal ECG. A patient with OMI can have a totally normal ECG!"
No prior exertional complaints of chestpain, dizziness, lightheadedness, or undue shortness of breath. He denied headache or neck pain associated with exertion. I sent this ECG to Dr. Smith, with the only information that it is a 17 year old with chestpain. 24 yo woman with chestpain: Is this STEMI?
All of the patients presented with chestpain , and they are all in triage. ECG#1 ECG#2 ECG#3 ECG#4 ECG#5 See outcomes of all 5 below, with the Queen of Hearts AI Bot interpretation. Triage is backed up, and 10 minutes into your shift one of the ED nurses brings your several ECG s that has not been overread by a physician.
A man in his 60's presented after 4 days of chestpain, with some increase of pain on the day of presentation. Exact pain history was difficult to ascertain. such Q-waves are associated with larger MI and worse outcomes (2. What complication is the patient with post-infarction regional pericarditis at risk for?
T-wave to ST ratio is greater than 4 in lead V6, making pericarditis unlikely (also there were no symptoms of pericarditis). It turns out that this was a 27 yo African American male who presented with pressure-like (non-pleuritic) chestpain and dyspnea. There is ST elevation diffusely: 2 mm in V2, 3.5 mm in V3, 2.5
A man in his 60's presented after 4 days of chestpain, with some increase of pain on the day of presentation. Exact pain history was difficult to ascertain. Although the patient has had pain for 4 days, could the artery have fully occluded only within hours? There was some SOB. Very unlikely. Raitt et al.) [and
A middle-aged woman had intermittent angina for 48 hours, then onset of constant, crushing chestpain for 1.5 Post-infarction Regional Pericarditis (PIRP) PIRP happens when MI is transmural, all the way from subendocardium to subepicardium, thus leading to inflammation of the subepicardium (next to the pericardium).
Apparently he denied chestpain. As always, takotsubo cardiomyopathy and focal pericarditis can mimic OMI, but takotsubo almost never mimics posterior MI, and both are diagnoses of exclusion after a negative cath. Could this outcome have been prevented with emergent cath? Here is his first ED ECG: What do you see?
Written by Jesse McLaren, with edits from Meyers Four patients presented with chestpain or shortness of breath, and ECGs labeled ‘inferior STEMI’. In addition, ischemic STD in aVL is highly sensitive for inferior OMI, and excludes pericarditis. Using principles of hyperacute T waves, do any have inferior occlusion MI?
Scenario 1 : The patient presents with 24 hours of substernal chestpain. The exception is with postinfarction pericarditis , in which a completed transmural infarct results in inflammation of the subepicardial myocardium and STE in the distribution of the infarct, and which results in increased STE and large upright T-waves.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




























Let's personalize your content